ABSTRACT
The stability of a dental prosthesis is its resistance to displacement when it is subjected to functional, horizontal and rotational stresses. For a removable partial denture (RPD), stability depends greatly on overall quality of fit to the supporting teeth and tissues. There are numerous reasons why the fit of a newly fabricated RPD might be compromised, but it is easy for the dentist to determine visually whether vertical movement is excessive. If finger pressure applied to the distal-most tooth on a distal extension denture base results in lifting of the anterior-most indirect retainer, then the RPD is not stable and either an indirect (laboratory processed) or direct (chairside) hard reline should be carried out. In this paper, we discuss factors that might influence the need to do a direct, chairside hard reline at delivery of a newly fabricated distal extension RPD and we recommend techniques.
Introduction
A removable partial denture (RPD) acts as a substitute for rather than a replacement of missing teeth and oral tissues. Thus, patients must adapt to both the presence of the prosthesis and any movement that occurs during function. Although not supported by any standard of patient satisfaction, we traditionally assume that the basic requirements of support, retention and stability must be met at the delivery appointment.1
Careful planning and optimization of the condition of abutment teeth and supporting tissues before taking the definitive impression should result in a relatively retentive prosthesis overlying a healthy foundation. However, achieving ideal stability (i.e., no movement during function) in a distal extension RPD may be impossible. The purpose of this paper is to discuss factors that might influence the need for a direct, chairside hard reline at time of delivery of a newly fabricated distal extension RPD and to recommend techniques.
What Is Stability and Why Is It Important?
The stability of a dental prosthesis is its resistance to displacement when it is subjected to functional, horizontal and rotational stresses. Support is provided by the foundation (teeth and soft tissue) on which the prosthesis rests.2 Unlike that of a fixed partial denture, which is anchored in a set position, RPD stability depends primarily on the overall quality of adaptation of the prosthesis to the foundation—both horizontally and vertically—as well as the inherent mobility of the teeth and soft tissue forming the foundation. Simply put, a non-stable RPD may be poorly fitting or lack support or both. If an RPD is solely tooth or implant supported and has a well-fitting, properly designed framework, stability should be relatively good. Even if a prosthesis relies primarily on soft tissue support, a well-fitting framework significantly limits movement in a horizontal plane (i.e., lateral movement).
The duplication of oral tissues and the fabrication of a well-fitting prosthesis that will substitute for teeth and gingiva require meticulous attention to detail. Rudd and Rudd3-5 analyzed the overall process and postulated 243 possible errors that can occur during RPD fabrication. Early errors in impression making and improper use of materials can result in an inaccurate master cast; then, assuming one is fortunate enough to avoid numerous potential pitfalls and produce a framework with an acceptable fit, processing, polishing and delivery errors by the dentist (over-relief of undercut areas and borders of the denture base) can easily result in a compromised fit of the prosthesis. Dunham and colleagues6 examined 50 frameworks fabricated for patients by a US Army dental laboratory and found that most framework rests did not contact intended tooth surfaces.
Vertical stability of the distal extension RPD depends somewhat on the fit of the framework, but even more on the extent of coverage and quality of adaptation of the denture base to the supporting tissues; thus, this must be tested in the mouth. If finger pressure applied to the distal-most tooth on the denture base results in lifting of the anterior-most indirect retainer, then the RPD is not vertically stable (Fig. 1). Lack of stability can indicate poor fit of the prosthesis to the supporting soft tissues, slight inherent movement (or compression) of those tissues or both. A simple procedure to determine the extent of adaptation of the prosthesis to the soft tissue can be carried out by applying a small amount of polyvinyl siloxane impression material (without using adhesive) to the tissue side of the denture base and placing the prosthesis in the mouth while holding the framework rests in a fully seated position. When the impression material has set, the RPD is removed and examined. Thick areas of material indicate space between the resin and soft tissue; the thinner the material, the better the prosthesis is adapted to the underlying tissue.
The importance of good tissue adaptation of the distal extension resin base is magnified the further force is applied away from the terminal abutment. Because occlusal forces result in rotation of the denture base as a fulcrum is established on the terminal abutment(s), the greatest pressure will be exerted at the distal-most support area. Perpetual reduction of the residual ridge after tooth loss is mediated by anatomical, metabolic and mechanical factors.7,8 It would seem prudent to minimize and broadly distribute pressure to reduce the contribution of mechanical factors at RPD delivery if rotational movement is detected. Depending on the design of the framework and clasp rigidity, rotational movement of the denture base can also impose non-axial forces that may be detrimental to a weak terminal abutment (Fig. 2).
 Figure 1: Test for RPD stability by applying finger pressure to the distal extension base and looking for lifting of the anterior-most rest (indirect retainer).
Figure 1: Test for RPD stability by applying finger pressure to the distal extension base and looking for lifting of the anterior-most rest (indirect retainer).
 Figure 2: Retainer broken from a terminal abutment by excessive rotational movement of a non-stable distal extension RPD.
Figure 2: Retainer broken from a terminal abutment by excessive rotational movement of a non-stable distal extension RPD.
Why Would a Newly Fabricated Distal Extension RPD Not Be Stable?
Unquestionably, many distal extension RPDs have been successfully fabricated from single-stage impressions using a wide range of methods. Even so, because an RPD framework fits the master cast differently than the abutment teeth and certain impression materials record hard and soft tissues with different degrees of accuracy, a secondary impression made with the framework in the mouth is necessary when placing a distal extension prosthesis.2,9,10 The logic behind this altered cast procedure (to ensure that the tooth–framework and framework–soft tissue relations are accurate) seems reasonable, but because more steps are required, they must be done carefully to avoid introducing additional fitting errors. Also, use of the altered cast procedure has not been shown to produce clinically superior results compared with single-stage impression procedures in terms of the fit and stability of distal extension RPDs.11
Regardless of how the master cast is derived and its accuracy, a small degree of error is introduced during processing. The vast majority of RPD denture bases are made with conventional pressure-packed, heat-cured poly (methyl methacrylate) resin, which shrinks about 6% during polymerization.12 Release of residual stress also results in slight distortion of the denture base (which is bulk or shape dependent) after removal of the RPD from the processing cast.13 Eventual water absorption by the resin causes a slight expansion that may compensate for some, but not all, of the distortion occurring during processing.
Although newer methods of polymerization have been shown to reduce shrinkage to about 3%, resin denture bases do not have an ideal, uniform fit to the supporting tissues.14-16 For a complete denture, a non-uniform but somewhat close adaptation of the intaglio surface is usually clinically acceptable (although a posterior palatal seal must be added for a complete maxillary denture), because the entire prosthesis moves as a single occluding unit.13 However, for a distal extension RPD, the tissue fit must be optimal to minimize rotation of the denture base, which imposes uneven pressure on the residual ridge and non-axial forces on the terminal abutment(s).
How Do You Choose Between an Indirect and Direct Reline Procedure?
When a distal extension RPD lacks vertical stability, either an indirect (laboratory processed) or direct (chairside) hard reline procedure should be considered. The first option requires making an impression, sending the prosthesis to a dental laboratory and delivering it at a subsequent appointment. While the impression is made, the patient should be instructed to move the lips and tongue to help border mould the material to establish the extent of the reline. The technician must be careful not to distort or damage the framework and be absolutely certain that the denture flask or reline jig is fully closed to prevent a change in the framework–tooth relation or the vertical dimension of occlusion.17 There is also a slight risk of distortion of the resin base due to processing heat.2 In addition, the technician may over-polish the lateral borders of the processed reline and produce an RPD that is under-extended. The occlusion, the fit of the framework and the extension of the borders should all be re-evaluated at the delivery appointment. The advantage of laboratory processing is a stronger, denser and more completely cured resin reline compared with direct reline materials.18 The disadvantages are the need for an extra appointment and the additional laboratory fee.
Craig and Powers18 listed 4 primary criteria for an RPD reline: a good chemical bond, satisfactory strength, no warping or dimensional change in the prosthesis and the procedure should take only a short time for the convenience of the patient. Other concerns related to direct reline materials include patient tolerance (taste, temperature, odour), colour stability, durability and ease of handling and polishing. Early methyl methacrylate-based direct reline materials had numerous problems and were described as “temporary expedients.”19 The reformulated chairside hard reline materials available today have been designed to reduce many of those problems.
A chairside hard reline procedure offers the practitioner the opportunity to correct a clinical problem on the spot at a relatively low cost and give the patient a clinically acceptable product that should last for a reasonable length of time depending on how the prosthesis is handled. The disadvantage is that the materials used are somewhat inferior to heat-cured resins because they are less hard, more porous and flexible and less colour stable. They are also polymerized to a lesser degree, which may expose the patient to residual monomer potentially irritating the oral mucosa and causing a low-grade allergic response.18-23 Although both heat-cured processed and low-temperature non-processed resins always contain some residual monomer that can be cytotoxic to a degree depending on the particular patient, the latter presents a greater risk because of less polymerization. However, the risk to patients’ health is considered to be low.22 The many choices of hard, direct reline materials include auto-polymerizing, light- and dual-cured options. Light-cured materials are typically more completely cured and may expose the patient to fewer unreacted chemical components.
For both indirect and direct reline procedures, the denture base should be sufficiently relieved (~1 mm) to allow the impression or reline material to flow freely and form a uniform layer (Fig. 3).17 For a direct reline, the use of surface primers (monomers or organic solvents commonly supplied with individual products) cause the substrate resin to swell, which improves the bonding strength of the reline material (Fig. 4).24,25 A direct reline material should also flow easily to minimize distortion of the soft tissues and set completely within a reasonable time to allow for finishing (Figs. 5 and 6).
 Figure 3: About 1 mm of resin must be removed from the denture base before carrying out a chairside hard reline to allow for flow and uniform thickness of material.
Figure 3: About 1 mm of resin must be removed from the denture base before carrying out a chairside hard reline to allow for flow and uniform thickness of material.
 Figure 4: Applying specific monomers or organic solvents (supplied with the reline product) after reduction of the denture base improves bonding of the hard reline material.
Figure 4: Applying specific monomers or organic solvents (supplied with the reline product) after reduction of the denture base improves bonding of the hard reline material.
 Figure 5: For optimal results, material used in a direct chairside reline procedure should be free flowing and used according to the manufacturer’s instructions (GC Reline, GC America, Alsip, IL shown here).
Figure 5: For optimal results, material used in a direct chairside reline procedure should be free flowing and used according to the manufacturer’s instructions (GC Reline, GC America, Alsip, IL shown here).
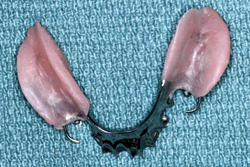 Figure 6: The tissue-contact surface of a direct, chairside hard reline fully polymerized before finishing.
Figure 6: The tissue-contact surface of a direct, chairside hard reline fully polymerized before finishing.
What Technique Should Be Used for a Direct Reline (or Reline Impression)?
Christensen26 has described a closed-mouth impression technique using a high-viscosity impression material to facilitate an indirect RPD reline that yielded a near optimal fit. In our opinion, a closed-mouth procedure should be used cautiously, because it can allow rotation of the distal extension base if the patient does not close exactly into the desired occlusion or if the impression material does not provide sufficient resistance to keep the anterior rests fully seated. Depending on the viscosity and flow of the impression or reline material, occluding the RPD could even over-compress the soft tissues and result in slight lifting of the most posterior rests during non-function.
The best way to ensure that all rests remain fully seated during a reline impression or a direct reline is for the dentist to hold the framework in place during the entire procedure, or at least until the material begins to set.27 As for the impression procedure for a laboratory reline, the patient should be instructed to move the tongue and lips to facilitate limited border moulding of the reline material. For best results and to reduce the possibility of difficult removal of the prosthesis, final polymerization of direct reline materials should be completed out of the mouth following the manufacturer’s specific instructions. After the reline (either indirect or direct) is complete, the occlusion should be re-evaluated and adjusted if a slight change has occurred. The borders should also be checked using a material such as pressure-indicating paste to ensure they are not over-extended. The ultimate goal is to achieve optimal soft tissue support in harmony with an ideal tooth–framework relation and a vertically stable distal extension RPD.27 For a removable prosthesis, the reline should be evaluated periodically (every 6 months or less depending on the patient) to ensure that it has not degraded and to determine whether tissue changes warrant a new reline procedure.
We believe that any movement of an RPD during function is undesirable. We concede that occasionally the use of a “permanent” soft, viscoelastic reline material is desirable to allow for engagement of undercuts and coverage of non-attached mucosa or to better distribute functional forces; however, it allows for slight RPD movement. In general, these materials provide many advantages, but lack the durability, clean-ability, dimensional and colour stability and longevity of hard reline materials.28 In our opinion, their use should not be arbitrary.
Conclusion
From a biological and mechanical point of view, optimal support, retention and stability are desirable at delivery of any RPD. For the newly fabricated distal extension RPD, there are numerous reasons why stability might be compromised. Although less than ideal, if deemed necessary, a direct, chairside hard reline procedure may be the simplest, most practical and accurate treatment option to ensure that a patient (and customer) receives a vertically stable prosthesis.
THE AUTHORS
|
Dr. Hill is a professor in the department of care planning and restorative sciences, University of Mississippi School of Dentistry, Jackson, Mississippi. |
|
|
Dr. Rubel is a professor in the department of care planning and restorative sciences, University of Mississippi School of Dentistry, Jackson, Mississippi. |
Correspondence to: Dr. Edward E. Hill, Department of care planning and restorative sciences, University of Mississippi School of Dentistry, 2500 North State St., Jackson, Miss. 39216, USA. Email: eehill@umc.edu
The authors have no declared financial interests in any company manufacturing the types of products mentioned in this article.
This article has been peer reviewed.
References
- Frank RP, Brudvik JS, Leroux B, Milgrom P, Hawkins N. Relationship between the standards of removable partial denture construction, clinical acceptability, and patient satisfaction. J Prosthet Dent. 2000;83(5):521-7.
- Carr AB, McGivney GP, Brown DT. McCracken's removable partial prosthodontics. 11th ed., St. Louis, MO: Mosby, Inc.; 2005. p. 8.
- Rudd RW, Rudd KD. A review of 243 errors possible during the fabrication of a removable partial denture: part I. J Prosthet Dent. 2001;86(3):251-61.
- Rudd RW, Rudd KD. A review of 243 errors possible during the fabrication of a removable partial denture: part II. J Prosthet Dent. 2001;86(3):262-76.
- Rudd RW, Rudd KD. A review of 243 errors possible during the fabrication of a removable partial denture: part III. J Prosthet Dent. 2001; 86(3): 277-88.
- Dunham D, Brudvik JS, Morris WJ, Plummer KD, Cameron SM. A clinical investigation of the fit of removable partial denture prosthesis clasp assemblies. J Prosthet Dent. 2006;95(4):323-6.
- Atwood DA. Reduction of residual ridges: a major oral disease entity. J Prosthet Dent. 1971;26(3):266-79.
- Winkler S. Essentials of complete denture prosthodontics. 2nded., Littleton, MA: PSG Publishing, Inc.; 1988. p. 22-38.
- Principles, concepts, and practices in prosthodontics - 1994. Academy of Prosthodontics. J Prosthet Dent. 1995;73(1):73-94.
- Feit DB. The altered cast impression technique revisited. J Am Dent Assoc. 1999;130(10):1476-81.
- Frank RP, Brudvik JS, Noonan CJ. Clinical outcome of the altered cast impression procedure compared with use of a one-piece cast. J Prosthet Dent. 2004;91(5):468-76.
- O'Brien WJ. Dental materials and their selection. 3rd ed., Chicago: Quintessence Publishing, Inc.; 2002. p. 74-89.
- Woelfel JB, Paffenbarger GC, Sweeney WT. Dimensional changes occurring in dentures during processing. J Am Dent Assoc. 1960;61:413-30.
- Takamata T, Setcos JC. Resin denture bases: review of accuracy and methods of polymerization. Int J Prosthodont. 1989;2(6):555-62.
- Keenan PL, Radford DR, Clark RK. Dimensional change in complete dentures fabricated by injection molding and microwave processing. J Prosthet Dent. 2003;89(1):37-44.
- Teraoka F, Takahashi J. Controlled polymerization system for fabricating precise dentures. J Prosthet Dent. 2000;83(5):514-20.
- Brudvik JS. Advanced removable partial dentures. Chicago: Quintessence Publishing, Inc.; 1999. p. 101-3.
- Craig RG, Powers JM. Restorative dental materials. 11th ed., St. Louis, MO: Mosby, Inc.; 2002. p. 636-67.
- Bunch J, Johnson GH, Brudvik JS. Evaluation of hard direct reline resins. J Prosthet Dent. 1987;57(4):512-9.
- Williams DR, Chacko D. Jagger DC, Harrison A. Reline materials — handle with care? An investigation into the effect of varying the powder/liquid ratio on some properties of auto-polymerising acrylic resin materials. Prim Dent Care. 2001;8(4):151-5.
- Murata H, Seo RS, Hamada T, Polyzois GL, Frangou MJ. Dynamic mechanical properties of hard, direct denture reline resins. J Prosthet Dent. 2007;98(4):319-26.
- Hong G, Murata H, Li Y, Sadamori S, Hamada T. Influence of denture cleansers on color stability of three types of denture base acrylic resin. J Prosthet Dent. 2009;101(3):205-13.
- Jorge JH, Giampalo ET, Machedo AL, Vergani CE. Cytotoxity of denture base acrylic resins: a literature review. J Prosthet Dent. 2003;90(2):190-3.
- Mutluay MM, Ruyter IE. Evaluation of adhesion of chairside hard relining materials to denture base polymers. J Prosthet Dent. 2005;94(5):445-52.
- Leles CR, Machado AL, Vergani CE, Giampaolo ET, Pavarina AC. Bonding strength between a hard chairside reline resin and denture base material as influenced by surface treatment. J Oral Rehabil. 2001;28(12):1153-7.
- Christensen GJ. Relining, rebasing partial and complete dentures. J Am Dent Assoc. 1995;126(4):503-6.
- Phoenix RD, Cagna DR, DeFreest CF. Stewart's clinical removable partial prosthodontics. 3rd ed., Chicago: Quintessence Publishing, Inc.; 2003. p. 462-5.
- Braden M, Wright PS, Parker S. Soft lining materials — a review. Eur J Prosthodont Restor Dent. 1995;3(4):163-74.