Abstract
In this case report, we describe the successful long-term treatment of a patient with dental agenesis. The initial treatment plan included an orthodontic phase to provide adequate space for replacing missing lateral incisors with implants. However, because of some complications encountered after 2 years of orthodontic treatment, a revised treatment plan was considered to achieve functional and esthetic goals. The patient was completely satisfied 5 years after being treated with two 2-unit cantilevered resin-bonded fixed partial dentures supported by the cuspids. This conservative treatment plan was cost-effective without having any significant biological cost.
Clinical Significance
The 2-unit cantilevered resin-bonded fixed partial denture is a treatment option for replacing missing lateral incisors when clinical complications require modification of the initial treatment plan with implant-supported restorations.
Congenital absence of the maxillary lateral incisor, the second-most common dental agenesis, affects about 1% to 2% of the world's population.1 This anomaly is commonly accompanied by the absence of the corresponding tooth on the contralateral side. Females are about 1.4 times more prone to dental agenesis than males.1-3 Several factors such as genetic and developmental anomalies, systemic and local factors, trauma, and use of medication have been proposed as causal factors, but the definitive cause of this anomaly is not clear.1,4,5 Eighty-five percent of the expenditure related to the dental care of agenesis is for people who have up to 4 missing teeth.1
The chief complaint of most patients seeking prosthetic treatments because of congenital missing maxillary lateral incisors is having an unpleasant smile. To achieve an esthetic smile with minimal biological cost, a combined orthodontic-prosthodontic treatment plan is usually proposed. The goal is to create sufficient space to replace the missing lateral incisors by implant-supported crowns or to close the space by moving the canines into the lateral incisors' place and reshaping them with composite restorations.6-9 However, if any clinical complications occur, the patient could be offered an alternative or intermediate cost-effective treatment. The 2-unit cantilevered resin-bonded fixed partial denture could be a valuable treatment option in these situations. The case we reported here clearly illustrates this situation.
Clinical Case Presentation
A healthy 47-year-old woman was referred to the post-graduate prosthodontics clinic at the University of Montreal for a consultation about the possibility of using implant-retained restorations to replace her congenitally missing maxillary permanent lateral incisors. Her chief complaint was dissatisfaction with midline diastema (Fig. 1a). Her maxillary central incisors and canines were unrestored, had adequate crown height and width, and were free of periodontal diseases or mobility. Her maxillary lateral incisors sites had inadequate mesiodistal width and horizontal ridge atrophy. The patient had some defective restorations in her posterior teeth and generalized moderate marginal gingivitis, and pocket depths within normal limits. She also had loss of tooth substance, possibly attributable to attrition from parafunctional habits and erosion (Figs. 1b to 1d). The patient's medical history revealed that she was in good health and had no contraindications for implant surgery.
 Figure 1a: Intraoral frontal view showing dental agenesis and multiple diastemas.
Figure 1a: Intraoral frontal view showing dental agenesis and multiple diastemas.
 Figure 1b: Intraoral lateral view, right side.
Figure 1b: Intraoral lateral view, right side.
 Figure 1c: Intraoral lateral view, left side.
Figure 1c: Intraoral lateral view, left side.
 Figure 1d: Intraoral maxillary occlusal view.
Figure 1d: Intraoral maxillary occlusal view.
The treatment plan consisted of hygienic reinforcement, replacement of the defective restorations, a night guard and orthodontic treatment, followed by a bone graft to provide adequate mesiodistal and anteroposterior width of the edentulous space, and replacement of the lateral incisors with 2 implant-supported crowns.
After 2 years of orthodontic treatment with adequate retention time, the spacing for implant placement was adequate. However, the radiograph showed external root resorption, and clinical examination, mobility type II on the central incisors (Fig. 2a). We verified a lack of any traumatic occlusion and made sure that the patient wore her night guard. After an endodontic consultation, we told the patient that her maxillary central incisors were still vital (Fig. 2b), but that because of excessive orthodontic movements, she faced the potential risks of necrosis, progression of root resorption and ultimately extractions in the future.
 Figure 2a: Periapical radiograph showing mild external root resorption after 2 years of orthodontic treatment.
Figure 2a: Periapical radiograph showing mild external root resorption after 2 years of orthodontic treatment.
 Figure 2b: Intraoral frontal view after orthodontic treatment showing space redistribution.
Figure 2b: Intraoral frontal view after orthodontic treatment showing space redistribution.
Considering the clinical situation, we offered the patient several prosthodontic treatment plans. One option was to keep the central incisors and replace the lateral incisors as planned with implant-supported single-tooth restorations or with 2-unit cantilevered resin-bonded fixed partial dentures. Another option was to remove the central incisors and replace the missing teeth with a 4-unit implant-supported bridge or a 6-unit tooth-supported bridge.
We explained the advantages, complications and costs associated with all the options to the patient. At this point, the patient decided to avoid the bone-graft surgery with the placement of 2 implants and opted for a 2-unit cantilevered resin-bonded fixed partial denture in each quadrant. She was aware of the risks and limitations of resin-bonded fixed partial dentures (e.g.s, debonding of the framework from the abutment teeth and fracture of pontic). We thought that this treatment was a good option since we could follow the patient over time and change the restorations with minimal biological and financial costs, if needed.
Clinical Procedures
Before preparing the teeth, we did a diagnostic wax-up on mounted study models and had digital photographs with the reference shade tabs taken.
We splinted the maxillary central incisors with a lingual wire-composite (Filtek Supreme Universal Restorative, 3M-ESPE, St. Paul, MN) splint (Fig. 3). We followed the classical principles for conservative supra-gingival tooth preparations for a cantilevered resin-bonded fixed partial denture: minimally invasive lingual preparation limited to enamel (0.5 mm), resistance form (lingual chamfer and proximal groove) and maximum covering of the lingual surface area (Fig. 4).
 Figure 3: Wire-composite splint located at the middle third of loosened central incisors to stabilize the teeth.
Figure 3: Wire-composite splint located at the middle third of loosened central incisors to stabilize the teeth.
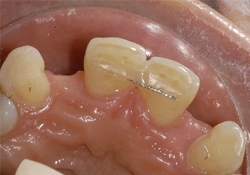 Figure 4: Palatal view of intra-enamel tooth preparations on both maxillary canines for cantilevered resin-bonded fixed partial denture.
Figure 4: Palatal view of intra-enamel tooth preparations on both maxillary canines for cantilevered resin-bonded fixed partial denture.
We made a complete final impression of the arch with polyvinyl siloxane elastomeric impression material (heavy body and low viscosity, Aquasil, Dentsply/Caulk, Milford, DE). We then fabricated the frameworks and the cantilevered bridges on the mounted master cast on an articulator (Fig. 5). At the try-in appointment, we assessed the complete seating of the frameworks, marginal adaptation, pontics' form and gingival pressure, esthetics and occlusion. We sent the bridges to the laboratory for final porcelain polishing and metal etching. At the final appointment, we used a dual-cured resin luting agent (Panavia 21OP, Kurary Co. Ltd, Osaka, Japan), for cementation and made minor occlusion adjustments.
 Figure 5: The 2 two-unit cantilevered resin-bonded fixed partial dentures on the master cast.
Figure 5: The 2 two-unit cantilevered resin-bonded fixed partial dentures on the master cast.
Follow-up
The patient was very satisfied with the treatment received and the final results (Figs. 6a and 6b). Over a 5-year follow-up period, her clinical condition remained stable and without complication (Fig. 7).
 Figure 6a: Post-treatment intraoral view showing the 2 two-unit cantilevered resin-bonded fixed partial dentures cemented.
Figure 6a: Post-treatment intraoral view showing the 2 two-unit cantilevered resin-bonded fixed partial dentures cemented.
 Figure 6b: Post-treatment full smile view showing completed treatment.
Figure 6b: Post-treatment full smile view showing completed treatment.
 Figure 7: Post-treatment clinical photograph at 5 years' follow-up, occlusal view.
Figure 7: Post-treatment clinical photograph at 5 years' follow-up, occlusal view.
Discussion
The case we report here is an example of the type of complications clinicians could encounter in their practice. In such situations, a total management plan should include dental and oral assessment, evaluation of the patient's complaints, needs, and socioeconomic status, and an evidence-based prognostic assessment.
In this case, the patient chose the option of cantilevered resin-bonded fixed partial dentures as a prosthetic solution for the problem encountered. This type of conservative treatment allows practitioners to evaluate the clinical condition over time, while offering the patient acceptable restorations. The predictability and longevity of this prosthetic design is less than conventional fixed bridges, but they are more reliable and less expensive than conventional resin-bonded fixed partial dentures with 2 abutments.10 Moreover, they offer better esthetics, easy cleaning, less biological damage and no chance of having an undetected debonded retainer with decay underneath it.11,12 In fact, the difference in the mobility of 2 abutments in the case of 3-unit resin-bonded fixed partial dentures can increase the risk of debonding.13-15 According to the literature, the success rate for 2-unit cantilevered resin-bonded restorations with a follow-up of at least 2 years is about 95%.10 The quality of life of people wearing this type of bridge is, moreover, no different than that of those with implants.16 This case report of a successful treatment with this type of restoration, followed up over 5 years supports this evidence.
Conclusions
Two-unit cantilevered resin-bonded fixed partial dentures can replace missing lateral incisors when a patient has clinical problems with the initial prosthodontic-orthodontic treatment plan. Full assessment of the patient's oral conditions, needs and preferences; regular check-up visit; and the patient's awareness of all treatment options, benefits, and potential risks and complications are essential parts of this management plan.
THE AUTHORS
|
|
Dr. Emami is assistant professor, department of restorative dentistry, faculty of dentistry, University of Montreal, Montreal, Quebec. |
|
|
Dr. St-Georges is associate professor, department of restorative dentistry, faculty of dentistry, University of Montreal, Montreal, Quebec. |
|
|
Dr. de Grandmont is associate professor, department of restorative dentistry, faculty of dentistry, University of Montreal, Montreal, Quebec. |
Correspondence to: Dr. Elham Emami, Oral health and rehabilitation research unit, Faculty of dentistry, University of Montreal, C.P. 6128, downtown branch, Montreal, QC. Email: Elham.emami@umontreal.ca
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Polder BJ, Van't Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta-analysis of the prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32(3):217-26.
- Stamatiou J, Symons AL. Agenesis of the permanent lateral incisor: distribution, number and sites. J Clin Pediatr Dent. 1991;15(4):244-6.
- Nik-Hussein NN. Hypodontia in the permanent dentition: a study of its prevalence in Malaysian children. Aust Orthod J. 1989;11(2):93-5.
- Woolf CM. Missing maxillary lateral incisors: a genetic study. Am J Hum Genet. 1971;23(3):289-96.
- Zilberman Y, Cohen B, Becker A. Familial trends in palatal canines, anomalous lateral incisors, and related phenomena. Eur J Orthod. 1990;12(2):135-9.
- Armbruster PC, Gardiner DM, Whitley JB Jr., Flerra J. The congenitally missing maxillary lateral incisor. Part 2: assessing dentists' preferences for treatment. World J Orthod. 2005;6(4):376-81.
- Armbruster PC, Gardiner DM, Whitley JB, Jr., Flerra J. The congenitally missing maxillary lateral incisor. Part 1: esthetic judgment of treatment options. World J Orthod. 2005;6(4):369-75.
- Richardson G, Russell KA. Congenitally missing maxillary lateral incisors and orthodontic treatment considerations for the single-tooth implant. J Can Dent Assoc. 2001;67(1):25-8.
- Sclar AG, Kannikal J, Ferreira CF, Kaltman SI, Parker WB. Treatment planning and surgical considerations in implant therapy for patients with agenesis, oligodontia, and ectodermal dysplasia: review and case presentation. J Oral Maxillofac Surg. 2009;67(11 Suppl):2-12.
- Wyatt CC. Resin-bonded fixed partial dentures: what's new? J Can Dent Assoc. 2007;73(10):933-8.
- van Dalen A, Feilzer AJ, Kleverlaan CJ. A literature review of two-unit cantilevered FPDs. Int J Prosthodont. 2004;17(3):281-4.
- Briggs P, Dunne S, Bishop K. The single unit, single retainer, cantilever resin-bonded bridge. Br Dent J 1996;181(10):373-9.
- Chan AWK, Barnest IE. A prospective study of cantilever resin-bonded bridges: An initial report. Aust Dent J 2000;45(1):31-6.
- Chai J, Chu FCS, Newsome PRH, Chow TW. Retrospective survival analysis of 3-unit fixed-fixed and 2-unit cantilevered fixed partial dentures. J Oral Rehab 2005;32(10):759-65.
- Botelho MG, Leung KCM, Ng H, Chan K. A retrospective clinical evaluation of two-unit cantilevered resin-bonded fixed partial dentures. J Am Dent Assoc 2006;137(6):783-8.
- Sonoyama W, Kuboki T, Okamoto S, Suzuki H, Arakawa H, Kanyama M, et al. Quality of life assessment in patients with implant-supported and resin-bonded fixed prosthesis for bounded edentulous spaces. Clin Oral Implants Res. 2002;13(4):359-64.