Abstract
Oral manifestations of chronic graft-versus-host disease (cGVHD) are a potentially significant complication of allogeneic hematopoietic stem cell transplantation. Oral cGVHD mucosal lesions often have a lichenoid appearance but may be erosive and extremely symptomatic. This clinical report highlights the use of topical corticosteroids for management of symptomatic oral cGVHD.
This brief report highlights the utility of topical corticosteroids in the management of oral chronic graft-versus-host-disease (cGVHD). A 50-year-old Asian female who had received an allogeneic hematopoietic stem cell transplant (HSCT) for undifferentiated acute leukemia presented 8 months post-transplantation for evaluation of symptomatic oral lesions of three weeks duration. She stated the lesions were extremely painful and interfered with routine masticatory functions, resulting in weight loss. The patient also reported recent onset of symptomatic vaginal lesions diagnosed as GVHD by her gynecologist. The patient’s gynecologist had prescribed systemic antivirals, antifungals and corticosteroids for the vaginal lesions without significant benefit for her symptoms.
Clinical examination of the oral cavity revealed multiple areas of ulceration with significant erythema on the buccal and labial mucosa bilaterally (Fig. 1). The clinical diagnosis was consistent with oral cGVHD given the patient’s history of allogeneic HSCT, clinical presentation of the oral lesions and concurrent diagnosis of genital GVHD. The patient was prescribed the following medication regimen: a) topical dexamethasone rinse 0.5 mg/5 ml (10 ml swish, 5-minute dwell time, and spit; 3 times daily) in order to achieve contact of medication with all mucosal surfaces, b) topical betamethasone gel 0.05% for direct application to ulcerative lesions (apply thin layer to accessible oral ulcers 3 times daily) and c) nystatin rinse 100 000 units/ml (5 ml swish and spit; 4 times daily) as antifungal prophylaxis. Upon 1-month re-evaluation, the patient stated she followed the medication regimen meticulously and was now completely asymptomatic. She reported regaining normal masticatory function shortly after starting the medication regimen and experienced associated weight gain. She also reported improvement of her vaginal condition with topical corticosteroid treatment as per her gynecologist’s recommendations. Clinical examination revealed complete resolution of her oral lesions (Fig. 2). The patient was instructed to use the previously prescribed topical medication regimen as needed if her oral lesions returned. When considering the current status of her oral condition, the patient stated, “it was like it never happened.”
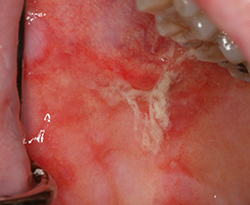 Figure 1: Significant erythema and ulceration of the right buccal mucosa consistent with oral chronic graft-versus-host disease (cGVHD). The patient had multiple lesions throughout her buccal and labial mucosa bilaterally with a similar clinical appearance.
Figure 1: Significant erythema and ulceration of the right buccal mucosa consistent with oral chronic graft-versus-host disease (cGVHD). The patient had multiple lesions throughout her buccal and labial mucosa bilaterally with a similar clinical appearance.
 Figure 2: Complete resolution of oral cGVHD lesions on the right buccal mucosa with a similar appearance on all mucosal surfaces that were previously affected.
Figure 2: Complete resolution of oral cGVHD lesions on the right buccal mucosa with a similar appearance on all mucosal surfaces that were previously affected.
Oral cGVHD usually occurs approximately 100 days post-HSCT in more than 70% of individuals who develop systemic cGVHD.1 The most common organ systems affected by systemic cGVHD are the skin, gastrointestinal tract and liver.1 Clinical manifestations of oral cGVHD often include striae, erythema and/or ulceration of mucosal surfaces, which are often symptomatic.1-4 Salivary gland dysfunction and pain are also common features of oral cGVHD.1-4 Systemic immunomodulatory agents are usually successful in treating systemic cGVHD; however, symptomatic oral cGVHD is often recalcitrant to these therapies and can be difficult to manage. Topical corticosteroids, such as those described in this report, have been shown to be of significant benefit for patients with symptomatic oral cGVHD.2‑4 Topical corticosteroids may be compounded with other medications, such as an antifungal agent, in order to increase compliance with the treatment regimen, especially in patients with functional or cognitive limitations, or both. Oral health care providers should consider topical corticosteroid therapy for patients with symptomatic oral cGVHD as described in the present case.
THE AUTHOR
 |
Dr. Stoopler is associate professor of oral medicine and director, oral medicine residency program, department of oral medicine, University of Pennsylvania School of Dental Medicine, Philadelphia, Pennsylvania. |
Correspondence to:Dr. Eric T. Stoopler, University of Pennsylvania School of Dental Medicine, 240 South 40th St, Philadelphia, PA 19104, USA. Email: ets@dental.upenn.edu
The author has no declared financial interests.
This article has been peer reviewed.
References
- Treister NS, Cook EF Jr, Antin J, Lee SJ, Soiffer R, Woo SB. Clinical evaluation of oral chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2008; 14(1):110-5.
- Imanguli MM, Alevizos I, Brown R, Pavletic SZ, Atkinson JC. Oral graft-versus-host disease. Oral Dis. 2008;14(5):396-412.
- Schubert MM, Correa ME. Oral graft-versus-host disease. Dent Clin North Am. 2008; 52(1):79‑109.
- Meier JKH, Wolff D, Pavletic S, Greinix H, Gosau M, Bertz H, et al. Oral chronic graft-versus-host disease: report from the International Consensus Conference on clinical practice in cGVHD. Clin Oral Invest. 2011;15(2):127-39.