
ABSTRACT
Dentistry is a profession that involves the acquisition and maintenance of fine psychomotor skills. The many components of the motor system in the brain work together during all movements, but each area is activated to a varying degree depending on whether an individual is learning, training or maintaining expertise. The transition from nonexpert to expert involves practice and experience to allow imprinting of neuronal connections within the brain, which in turn causes those practised movements to become automated. With age, many people slowly lose memory, but are the fine motor movements that a dentist has mastered over a lifetime also lost? The aging expert experiences the same deterioration as an aging nonexpert in tasks that are unrelated to the expertise, but tasks that an expert has selectively maintained through decades of practice are retained through aging.
Introduction
Dentistry involves the acquisition and maintenance of specific fine motor skills. The precise handedness and manual dexterity required to accomplish complex sensorimotor hand movements parallels the regulation of such activities by the brain. How do acquisition and maintenance of psychomotor skills occur and how can this process be optimized? The answers to these questions are relevant to professions such as dentistry, and dental schools may consider them when designing their curricula.1 This paper begins with an introduction to the neurologic regulation of motor activity by the brain, followed by a review of how psychomotor skills are acquired. Finally, we discuss how psychomotor skills that have been mastered by the dentist earlier in life are retained with age.
Motor Activity in the Brain: An Introduction
Much research has focused on identifying and understanding the specialized parts of the brain that control motor activity. Techniques that allow researchers to visualize brain activity during motor tasks include functional magnetic resonance imaging (fMRI) and repetitive transcranial magnetic stimulation. The areas of the brain involved in fine motor movements include the primary motor cortex, premotor cortex, presupplementary cortex and basal ganglia, supplementary cortex, posterior parietal cortex and cerebellum (Fig. 1)2-4:
- The primary motor cortex is organized in an orderly manner called somatotopic organization where each area represents and controls a specific and different part of the body. It is involved in force generation, task-specific muscle movements and automaticity of learned movements.
- The premotor cortex is vital in movement planning, execution and recognition of limb movements at the initial stages of learning psychomotor skills.
- The basal ganglia are active during voluntary movements that are not automated, and the presupplementary motor area is active when new sequences are being learned.
- The supplementary motor area allows self-initiation of movements, sequencing of previously memorized movements, 2-handed coordination and planning of complex movements.
- Visual feedback of limb movements is directed from the posterior parietal cortex (and the premotor cortex) to the primary motor cortex.
- The cerebellum controls the coordination, timing and accuracy of movements.
All these areas of the brain have individual roles but work together to fine-tune motor movements. They are activated to varying degrees depending on which stage–learning, training or expertise retention–a person is experiencing.
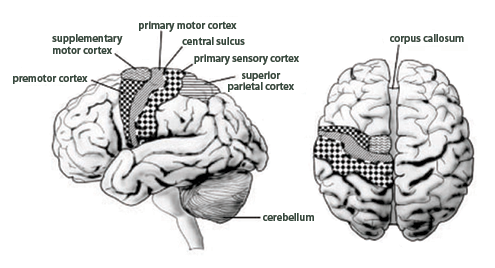 Figure 1: Location of the areas of the brain involved in fine motor movements. Right hand movements are controlled by the left side of the brain, and vice versa. The corpus callosum facilitates coordination and communication between the 2 sides of the brain. Note that the basal ganglia are not illustrated in this diagram as they form an internal structure within the brain. (Image reproduced with permission of Blackwell Publishing Ldt.4)
Figure 1: Location of the areas of the brain involved in fine motor movements. Right hand movements are controlled by the left side of the brain, and vice versa. The corpus callosum facilitates coordination and communication between the 2 sides of the brain. Note that the basal ganglia are not illustrated in this diagram as they form an internal structure within the brain. (Image reproduced with permission of Blackwell Publishing Ldt.4)
Acquisition of Fine Psychomotor Skills
Acquisition in the Nonexpert
The establishment of sensorimotor handedness depends largely on the limitations in controlling intricate finger movements. Many of these limitations are more obvious in the initial stages of learning and become less prominent with practice and long-term training.4-6 When a fine motor sequence of hand movements is performed for the first time, the premotor and presupplementary motor areas of the brain are maximally activated to extensively plan attempted movements that are perceived as a foreign experience.3-5,7 Activity in the primary motor cortex is maximal in only the first 7–14 minutes, then decreases.4-6
It has been hypothesized that this initial increased activity reflects the concentration and planning needed to activate and coordinate various muscles specific to the task. Furthermore, many studies have observed, using fMRI, that activity in the basal ganglia can only be detected at the early stages of acquisition.4-6
In contrast to the increase in activity in these areas, there is considerably less activity in the supplementary motor cortex and very diffuse activity in the cerebellum during acquisition.2,4-6 In summary, planning of novel movements requires much activity and stimulation of the central nervous system to complete a task successfully.
Acquisition in the Expert
Everyone knows the cliché “practice makes perfect,” but how? It appears that plasticity (the ability of the brain to adapt in response to a stimulus) plays a significant role in turning an amateur into an expert.8 In well-practised and trained professionals, movement sequences, even complex ones, have become automated; the expert employs previously established neuronal connections instead of creating new connections with each motor sequence performed (as would the nonexpert).2,4-7 Hence, the intensity and amount of activity stimulated in the brain of an expert are less, more highly focused and much more rapid than in a nonexpert.
The centre of activity is highly concentrated in the primary motor cortex, and this high level of activity does not diminish over time during execution of movement sequences; in the nonexpert, activity diminishes after 7–14 minutes.4,5,7 For a movement that has become automated due to practice in the expert, the constant high activity level in the primary motor cortex is mainly due to the automaticity of the movements.4,6 Automaticity reflects imprinting of information within the brain’s circuitry.2,4-7 As an indication of imprinting, Karni and colleagues6 found that there was already an observable increase in finger representation within the primary motor cortex on fMRI after only 30 minutes of practice; however, this activity diminishes within 1 week in the absence of regular training.6 Therefore, regular practice is needed to maintain the neuronal activities and connections involved in a specific activity until the information can be transferred from the premotor cortex and be imprinted in the primary motor cortex to develop automaticity.5,6,9 In fact, Ericsson and colleagues8 and Ericsson and Lehmann10 show that approximately 10 years of practice is required for the transition from a nonexpert to an expert.
However, no significant studies have been carried out to determine the duration and frequency of practice needed within these 10 years to ensure the transition. For example, would it be more effective if practice was scheduled for frequent short periods (e.g., 1 hour 4 times a week) or longer, less frequent periods (e.g., 3–4 hours once a week)? Such information would be beneficial for dental schools to consider when scheduling clinical simulation labs.
Also observed in professionals is an absence of activity in the basal ganglia, little activity in the premotor and presupplementary cortices and greater activity in the supplementary cortex.4,6 The activity in the supplementary motor area is associated with execution of sequences already memorized. Activity in the cerebellum is more localized and concentrated in the professional than in the amateur (Fig. 2).4,6
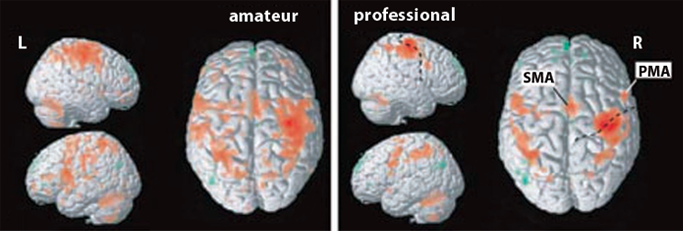 Figure 2: Functional magnetic resonance imaging of cortical activity in the brain of amateur and professional violinists during acquisition of fine motor movements. Cortical activity in the amateur is more diffuse, whereas activity in the professional is more focused and centred in the primary cortex and supplementary cortex. (SMA = supplementary motor area; PMA = premotor area). (Image reproduced with permission of Blackwell Publishing Ldt.4)
Figure 2: Functional magnetic resonance imaging of cortical activity in the brain of amateur and professional violinists during acquisition of fine motor movements. Cortical activity in the amateur is more diffuse, whereas activity in the professional is more focused and centred in the primary cortex and supplementary cortex. (SMA = supplementary motor area; PMA = premotor area). (Image reproduced with permission of Blackwell Publishing Ldt.4)
In addition to the gross anatomic changes mentioned above, many microstructural changes are also significant.2,7 The brain’s adaptation in establishing new neuronal connections involves increased myelination around axons of existing and newly forming neurons, which results in increased conduction velocity, an increased number of axonal collaterals and branches, a greater number of more stabilized synapses, increased neurotransmitters released within the same synapse resulting in increased precision and accuracy and greater recruitment of cortical matter.2,7 This ability of the brain to change and adapt in response to a stimulus, such as continuous practising, results in imprinting of neuronal connections, which allows these connections to be retained in the brain and, thereby, allows automation of the movements that result from these connections.
Retention of Fine Motor Skills in Professionals
Previous School of Thought: Slowing Models
With age, many people slowly lose memory, but are the fine motor movements that a dentist has mastered over a lifetime also lost? The older literature on maintenance of fine psychomotor skills is saturated with many “slowing models,” which suggest that both fine and gross motor skills deteriorate over time as part of the natural progression of aging; this concept is called the negative-age effect.6,8,11,12 One model states that, with age, there is an inevitable loss of neurons and neurotransmitters and, hence, an inevitable loss of neurologic function. 8,11,12 Another hypothesis is that with increasing age, there is a decrease in the signal-to-noise ratio due to a larger amount of “noise” within the brain that has the potential to interfere with normal neuronal connectivity. 8,11,12 A third model attributes age-related deterioration to decreases in protective antioxidant products that would normally help relieve oxidative stresses imposed on the brain by free radicals. These theories assume a generalized age-related decrement across all cortical processes.13
Many studies have hypothesized that this negative-age effect is applicable to all cognitive functions; however, these studies do not test age-related effects on the various parameters of cognition individually.8,11,12 More recent studies have attempted to disaggregate the components of fine psychomotor skills. Consequently, the slowing models have been challenged on the basis of being too vague and nonspecific. It may be possible that negative-age-related deterioration cannot be applied to all of the numerous cortical processes that are activated during any one task.8,11,12
Neurologic Concept of Savings
The concept of savings–postulated to be regulated by the cerebellum–dismisses and refutes the idea that deterioration of excitatory neuronal processes developed and reinforced throughout a lifetime of practice can simply disappear.2,14 According to this theory, for functional deterioration to occur, the brain must produce inhibitory pathways to oppose the excitatory pathways that have become embedded in the brain.2,14 The more practice an expert has had over longer periods of time, the more excitatory pathways have accrued in the brain, and the more inhibitory pathways are needed to cause “deterioration” in these pathways and subsequent “unlearning.”
Savings explains a familiar property of most learning systems: when things have been learned previously but not practised for some time, they are much quicker to relearn at a subsequent time, and, when things have been learned incorrectly, they are more difficult to “unlearn.”2,14 Intuitively, this is an important concept to emphasize to dental students as they begin to learn psychomotor skills. By extension, although learning new fine motor movements may be slow in the beginning, it is imperative that these skills be learned properly and under professional supervision to ensure that “good habits” are formed.
Current School of Thought
More recent literature has suggested that decreases in functioning capabilities with age may be applied to some parameters involved in the execution of fine motor skills, but not to all parameters. These studies separate fine psychomotor skills into 7 parameters: timing,8,11 sequencing,8,11,12 speed and precision of hand–eye coordination,11,15 visuospatial coordination,11,13 perception,16 memory9,10,16 and mechanical ability.11,13 Visuospatial coordination, perception and memory are considered more complex and higher executive processes within the brain. Some of these domains were evaluated separately from each other in relation to the effects of age.
Timing
It has been proposed that the cerebellum possesses a central timer or internal clock that relays information about the time between initiation of a movement within the cortical brain and the actual implementation of the task by the peripheral motor system.8,11 Therefore, continuous feedback to the cerebellum about any delay is necessary to allow the cerebellum to time movements correctly. Timing of movements, tested by executing a simple pattern of repetitive tapping, has been found comparable between healthy young adults and healthy older adults up to 80 years of age.8,11 This shows that lower-level timing processes are stable with increasing age, which suggests that simple tasks that depend primarily on such processes and less on higher executive processing are also preserved with age in both the expert and the nonexpert.8,11
Sequencing and Higher Executive Processes
In the nonexpert who is performing complex movement sequences, the intact lower-level timing processes of the cerebellum must interact with higher cortical structures and processes (visuospatial abilities, perception and memory), which are affected by age.8,11,12 As a result, the ability to sequence novel complex movements decreases with age in the nonexpert, resulting in delay of sequential movements as well as errors in the sequence itself.8,11,12 Because aging adults cannot rely on higher cortical processes, they increasingly rely on their intact lower-level timing centre for unfamiliar complex tasks, causing a simplification of these complex rhythmic sequences to prevent higher cortical processing from being overworked.12
With experts, it appears that familiar complex sequences do not decline with age.12 The expert has accumulated experience with specific complex sequences, which are now perceived in the brain as “simple” sequences that need less interaction with and depend less on higher cortical structures. These sequences are more automated and need only rely on lower-level timing processes, which, as mentioned above, remain intact with aging.8,11,12 Essentially, sequences that are complex are perceived as simple within the neurologic circuitry of an expert.
Speed and Precision
In experts, the speed and precision with which they perform skill-related tasks are maintained into later adulthood, with a slight decline in the seventh decade of life.11,15 However, both experts and nonexperts show reduced speed and accuracy in unfamiliar complex tasks unrelated to their expertise.11,15 This is partly explained by a neuropsychologic concept called “advance preparation” where cognitive processes have adapted to optimize task-related performance to a common peripheral environment.11,15 For example, a typist has optimized performance to the layout of the keyboard so that typing has become automated and sequences of letters are pressed almost simultaneously. Similarly, the pianist is optimized to the 88 keys of the piano. A dentist is optimized to his or her individual ergonomic hand positioning in relation to the anatomic and morphologic position, depth and strength of a tooth and the learned way to hold instruments. Speed and precision are very much related to the commonality of everything involved in a task-related process. Things that change commonality decrease speed and precision.11,15
Mechanical Ability
The effects of aging on mechanical ability relate to effects of aging on muscles, bones and the neuronal processes that innervate and regulate these structures. As this parameter requires more extensive research into both the neurologic and musculoskeletal systems, and as this paper deals only with the overall neurologic effects of aging on psychomotor skills, it is suggested that subsequent research can be done in this area.
Conclusion
Acquisition of fine motor skills involves many cortical structures in the brain, consisting of a multitude of neuronal processes and interactions. In an amateur, most of these structures are highly activated, but as the amateur becomes an expert, the sensorimotor skills and acquired dexterity become automatic and the brain requires less activity to carry out the same processes. The necessary neuronal connections have been imprinted in the brain and the tasks are, hence, perceived in the brain as simple. The aging expert experiences the same deterioration as an aging nonexpert in tasks that are unrelated to his or her expertise. But skill in the tasks that the expert has selectively maintained through accumulation of decades of practice is retained through aging.
The first implication of this is the importance of repetition and practice to facilitate imprinting of lifelong neuronal connections. However, not only practice, but also practising correctly is important, as “unlearning” bad habits is difficult. The second implication is that although skills are neurologically maintained through the aging process, expert dentists may still experience slowing in their performance due to deterioration of other factors, such as hearing, vision, etc. Therefore, it is just as imperative for dentists to maintain their hearing, vision and other functions to keep their skills up to speed as it is for them to practise. As mentioned above, the neurologic aspect of retaining expertise-related psychomotor skills with increasing age is only one component. The next step is to research the effects of aging on the musculoskeletal system and their implications for the aging dentist.
THE AUTHORS
|
Dr. Duong practises dentistry in Coquitlam and Surrey, British Columbia. At the time this article was written, she was a fourth-year dental student at the University of British Columbia, Vancouver, British Columbia. Email: janice.kt.duong@gmail.com |
|
|
Dr. Gardner is assistant clinical professor in the department of oral health sciences, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. |
|
|
Dr. Rucker is professor and chair of general dentistry in the department of oral health sciences, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. |
Correspondence to : Dr. Janice Duong, #1134 – 2929 Barnet Hwy, Coquitlam, BC V3B 5R5.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- De Andrés AG, Sánchez E, Hidalgo JJ, Diaz MJ. Appraisal of psychomotor skills of dental students at University Complutense of Madrid. Eur J Dent Ed. 2004;8(1):24-30.
- Altenmuller E, Gruhn W. Brain mechanisms. In: Parncutt R, McPherson G, editors. The science and psychology of music performance: creative strategies for teaching and learning. New York: Oxford University Press; 2002. p. 63-87.
- Gerloff C, Corwell B, Chen R, Hallett M, Cohen LG. The role of the human motor cortex in the control of complex and simple finger movement sequences. Brain. 1998;121(Pt 9):1695-709.
- Watson AH. What can studying musicians tell us about motor control of the hand? J Anat. 2006;208(4):527-42.
- Hund-Georgiadis M, von Cramon DY. Motor-learning-related changes in piano players and non-musicians revealed by functional magnetic-resonance signals. Exp Brain Res. 1999;125(4):417-25.
- Karni A, Meyer G, Jezzard P, Adams MM, Turner R, Ungerleider LG. Functional MRI evidence for adult motor cortex plasticity during motor skill learning. Nature. 1995;377(6545):155-8.
- Schlaug G. The brain of musicians: a model for functional and structural adaptation. Ann NY Acad Sci. 2001;930:281-99.
- Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100(3):363-406.
- Zec RF. The neuropsychology of aging. Exp Gerontol. 1995(3-4);30:431-42.
- Ericsson KA, Lehmann AC. Expert and exceptional performance: evidence of maximal adaptation to task constraints. Annu Rev Psychol. 1996;47:273-305.
- Krampe RT. Aging, expertise and fine motor movement. Neurosci Biobehav Rev. 2002;26(7):769-76.
- Salthouse TA, Babcock RL, Skovronek E, Mitchell DR, Palmon R. Age and experience effects in spatial visualization. Dev Psychol. 1990;26(1):128-36.
- Shukitt-Hale B. The effects of aging and oxidative stress on psychomotor and cognitive behavior. Age. 1999;22(1):9-17.
- Medina JF, Garcia KS, Mauk MD. A mechanism for savings in the cerebellum. J Neurosci. 2001;21(11):4081-9.
- Salthouse TA. The processing-speed theory of adult age differences in cognition. Psychol Rev. 1996;103(3):403-28.
- Kennedy KM, Partridge T, Raz N. Age-related differences in acquisition of perceptual-motor skills: working memory as a mediator. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2008;15(2):165-83.