Abstract
Background: Disparity exists between the public view of the "ideal" dentist and patient experiences of dental practice: dentists are expected to be altruistic and patient-centred, yet patient surveys suggest that the profession is overly motivated by profit.
Objective: To determine how the public views dental care in Quebec.
Methods: A random sample of comments about Quebec dentists made in 2011 was extracted from the public website RateMDs.com. Dentist characteristics and patient comments were analyzed using descriptive statistics and qualitative deductive and inductive thematic analysis.
Results: Eighty-six entries from a random sample of 47 of a possible 750 dentists were extracted and analyzed. Most dentists were men (66%) and worked in Montreal (51%). Patient comments were mainly positive (83%). Themes included overall impressions, communication and care, clinical competence, professionalism and office environment. Positive comments focused on patient-centred communication, in which the patient felt respected and involved in treatment planning; competence, seen as comprehensive, efficient and long-lasting treatment; and professionalism, which included ethical behaviour such as knowing professional limits. Negative comments focused on reticent communication styles that did not encourage patient input; incompetence, which included poor pain management and unnecessary treatment; and unprofessional conduct, such as lack of transparency in pricing.
Conclusion: In contrast with the negative image of dentists reported from patient surveys, comments on one public website were primarily positive. Our findings reinforce the importance of patient-centred education and communication training for students and continuing education.
Patient experience and satisfaction have become important components in the evaluation of the quality of health care.1-3Patient satisfaction has also been linked to clinical outcomes.4-6 In dentistry, important drivers of patient satisfaction are good communication and a patient-centred approach in which the patient feels listened to, respected, cared for and valued.2,7,8
According to dental literature, both the American and Canadian public are conflicted about the dental profession.9,10 On one hand, the public believes that dentistry should be a "noble, scientific-based profession comprised of caring individuals who always place the well-being of patients first."11 On the other, a recent Canadian Dental Association (CDA) survey suggests that "dentists are frequently viewed by patients as business people making treatment recommendations motivated more by profit than by the health needs of individual patients."10 Many dentists believe that patients value their work, but most (two-thirds) of the 3500 lay participants in the CDA survey did not agree that dentists provide good treatment value.10 Many questioned the motivation behind treatment recommendations, and almost 40% felt that dentists sometimes recommend unnecessary treatments. According to a member of the CDA's Board of Directors, "Quite simply, trust is built through patient communication. Dentists believe they are doing this. Patients tell us that we're not."10
Although this national survey provides an image of the Canadian public, dental associations and professional cultures also operate at a regional level. With the national portrait as a reference point, we endeavoured to determine how Quebec residents feel about their dental workforce; that is, what is truly important to people in Quebec during a dental encounter.
The Internet is becoming a popular source of health information12 and peer support for illnesses, including dental anxiety.13 Over the last decade, numerous websites have been developed to encourage health care consumers to evaluate publicly their health care experiences with individual practitioners. One goal of these sites is to enable peer-to-peer information sharing. Coined "physician rating sites," they are similar to other consumer information websites rating hotels, restaurants or electronic products, for example. They are consumer driven, and their free access, lay language and user friendliness using Web 2.0 make them more accessible than expert-driven approaches to health services reporting.3
Researchers,14-16 as well as professional associations,17,18 have become increasingly interested in what patients write on physician rating sites. Precedents are increasing for using these online data sources to understand patient satisfaction,3,14,16,18-21 including research showing an association with traditional measures of patient satisfaction.22
Although dental rating sites exist, the dental community has yet to publish an analysis of, or responses to, these ratings. This paper is one of the first to explore online patient comments about oral health professionals.
Methods
Data source: RateMDs (www.ratemds.com) is an international public website inviting user-generated commentary on health care professionals. RateMDs is among the oldest physician rating sites, and it is in the top 10 most frequently visited English-language rating sites.3,14,18,21 Users can search the ratings by a professional's name, gender, specialization and geographic region and leave anonymous comments; however, only 1 entry is permitted per professional per Internet protocol (IP) address. The site asks patients to rate the dentist using a 1–5 scale in the following categories: staff (poor to great); punctuality (not on time to on time); helpfulness (very unhelpful to very helpful); knowledge (unknowledgeable to knowledgeable). [Ed Note: The rating scales on the site have since changed to 'terrible', 'poor', 'okay', 'good' and 'excellent'] Comments are then solicited by the following request: "Please make your comments detailed and polite. Tell us WHY you rated as you did. This is not the place for reporting illegal activity unless you include a link to a website with supporting evidence. You are legally responsible for what you write here." User postings are moderated "to avoid libel or simply far-fetched statements."18
Design: A random sample of comments on RateMDs was extracted for dentists practising in Quebec and rated in 2011. To facilitate data extraction and random sampling, all dentists matching those criteria (n = 750) were listed alphabetically. All comments for the first 10 dentists were used to build the preliminary coding scheme; thereafter, comments for every 20th dentist were extracted. A coding scheme was developed by the first author (MEM) using the fields provided on the website in addition to a review of the dental education literature. Inductive themes emergent from the verbatim comments were then added as the coding progressed. Coding was done by the second author (AB) and verified by the first author (MEM).
After the sample comments were coded, the coding was assessed for informational redundancy. At this point the coding categories were saturated (i.e., no new codes emerged)23 so the sample size was not increased.
Coded data were then analyzed by the first author (MEM), who reviewed and combined codes with accompanying data into themes and subthemes. The second author (AB) reviewed these themes and subthemes and final interpretation was arrived at by consensus. Exemplar quotations were identified by both authors to illustrate the themes.
Descriptive statistics were used to classify dentist demographics (office location and gender) and the occurrence of positive versus negative patient comments.
Results
Comments on 47 dentists were extracted and analyzed; there were approximately 1.8 comments per dentist (n = 86 patient entries). Most dentists were male (66%) and most were working on the Island of Montreal (51%). This roughly reflects the dental workforce in Quebec: in 2011, 59% were male24 and 38% worked in Montreal.25
Thematic categories for comments included: positive versus negative valence; overall impression; communication and care; clinical competence; professionalism and office environment (Fig. 1). (Note: comments were in English and French; however, all examples are rendered here in English).
Positive Versus Negative Comments
A large majority of patient comments about their dentists were positive (83%). Negative comments were clustered mainly around 4 topics: time management, financial issues, knowledge and skills and professionalism (Fig. 1). Each negative topic was addressed by a minority of patients and solicited much positive commentary.
Overall Ratings
General phrases were commonly used to provide an overall impression of the dentists. Positive comments were most common (41 of 45 entries); for example: "I give him the highest rating," "Great dentist!," "I am very satisfied!," "We are incredibly blessed to have him." In some cases, the overall comments went further ("I have recommended him to friends and they are now likewise extremely satisfied customers"). Some ratings were qualified by comparisons with other dentists and clinics ("Could possibly be the best dentist in Canada") or the length of relationship ("Have been with her all my life").
At the other end of the spectrum, a minority of patients (4 of 45) provided overall descriptors with a negative valence, such as "Horrible dentist," "She is the worst dentist I have met" and "I remained in shock from his services."
Communication and Care
Communication and care emerged as the largest thematic domain. It included the following subthemes, each with positive and negative comments.
Patient education: Positive comments focused on patients' appreciation that the dentist explained procedures, including using illustrations to do so; that the dentist explained how the value of the treatment corresponded to the cost; that the dentist educated the patient without patronizing him or her; and that the dentist took time to clarify complicated procedures to reassure the patient. Negative comments in this domain focused on lack of education provided by the dentist and on contradictory diagnoses from the same dentist.
Patient involvement in treatment planning: Positive comments regarding treatment planning included dentists giving patients options; dentists speaking clearly about potential costs and consequences; and patients feeling that their needs and wishes were supported. Patients commented negatively when a dentist did not explain a procedure, did not seek patient input and did not listen to their requests or concerns.
Attitudes and behaviours: Positive descriptors of dentists' attitudes and behaviours included accommodating, attentive, caring, compassionate, friendly, gentle, gets to know the patient, helpful, available to listen, motivated, nice, passionate, patient, pleasant, reassuring, sense of humour, always smiling, inspires trust, a warm manner and welcoming. Patients were unhappy when dentists were not talkative, when they were impatient and when they did not offer what was considered "good" service.
Time management: Patients praised dentists for being available, efficient and punctual; for returning their calls promptly; for having acceptable waiting times; and for providing explanations when they were running late. Patients felt disrespected and that their own time was being wasted when the dentist was not punctual or organized.
Financial issues: Patients compared prices among dentists and commented on the quality of service in comparison to price; further, they appreciated dentists who assisted with insurance claims. Patients commented negatively on dentists they felt to be overcharging and those attempting to "sell" what they considered to be unnecessary products and services. Patients felt disrespected when the dentist charged more than other dentists.
Clinical Competence
Patients commonly used the term "competence" in writing about their impressions of their dentist. They judged clinical competence positively and negatively based on the following domains.
Knowledge and skills: Patients felt confident when they believed that their dentist was both knowledgeable and skillful. They commented positively if the dentist was "up-to-date" and "knows what he is doing." In contrast, patients were upset over poor-quality work (e.g., "He ruined the enamel on the whole tooth") and spoke about seeking second opinions after unsatisfactory care.
Pain: Pain appeared in the comments as a marker of skill. With a skillful dentist, for example, "You barely feel the needle." In contrast, incompetent dentists were seen to leave the patient in pain during and after the procedure.
Efficiency and effectiveness: Efficiency and effectiveness were used in the comments as markers of competence. Dentists concerned with durability and quality, those who do not do "any unnecessary work" and those who "resolve the problem quickly" were praised. Work that was not durable was criticized.
Comprehensive care, prevention and infection control: A concern about comprehensive care beyond oral health and a focus on prevention were seen to be positive attributes. Infection control standards were noted and appreciated.
Professionalism
Characteristics associated with professionalism in the dental education literature were present in the comments. The term "professional" was used to commend a dentist (e.g., "a true professional"). Ethical care was captured in comments describing dentists as working for the best interests of the patient and family, suggesting necessary treatments only and never pressuring patients to make decisions. Dentists who were honest about their own limits and referred patients to specialists when appropriate were praised. Polite, courteous dentists were appreciated. In contrast, "unprofessional" behaviour was also noted. For example, patients commented on dentists who "smelled like cigarettes" and who did procedures without discussing costs.
Office Environment
Patients commented on 3 main components of the office environment: the technology (old versus new), cleanliness and staff. Staff were described as attentive, caring, competent, excellent, fantastic, good, great, never without a smile, professional and wonderful. Bad attitudes were mentioned in few staff. High staff turnover was noted in 1 comment as a negative factor.
Discussion
Similar to reviews of physicians,14,15,21,26 most reviews of dentists were positive, countering a common contention that these sites are dominated by disgruntled patients.16 Although the dominance of positive commentary contrasts with the CDA survey noted above10, it corresponds with two recent British surveys in which patients' confidence and trust in their dental providers and their satisfaction with treatment were consistently high.7,27
Although in the minority, the negative comments are still important. Such remarks appeared in all areas: dentist–patient interaction (e.g., chair-side manner and time management), competence (e.g., pain) and systems issues (e.g., prices and office staffing).
Similar to the findings of Lopez and colleagues regarding physicians,26 our results suggest that interpersonal manner is important to patients. Positive comments focused on patient-centred communication that made patients feel cared for, listened to, respected, educated and involved in their treatment planning. This concurs with what the dental education literature claims patients seek2 and what the medical literature suggests is important in primary care outcomes.28,29
In contrast, negative comments in this domain related to what could be called "dentist-centred" communication, i.e., an approach that does not treat the patient as a valuable contributor to the relationship and treatment planning. Abrahamsson and colleagues30 found that strained communications and lack of trust between patient and dentist were associated with negative consequences, such as dental fear; studies also show the positive role that interpersonal communication plays in reducing dental anxiety.31,32Negative comments also focused on lack of competence, especially around pain control, and dental pain can lead to anxiety and fear as well.32
Although communication issues involving cultural and language barriers between patient and dentist have been reported to be major obstacles to oral health care,33-35 these did not appear in our data. Their absence is more likely a result of sampling bias than an indication that these issues are not important.
The CDA survey found that the public sees dentists as often motivated by profit.10 Similarly, a recent editorial in an American dental journal bemoaned the corporate image of the profession.9 How the public views the profession should not be regarded as a proxy for how patients view their personal relationship with their individual dentist. However, it is worth mentioning that, according to our data, patients feel that finances and profit affect the dental encounter. Of the 12 comments that discussed financial issues, 7 were positive.
Patients in our sample appreciated value and transparency. They wanted prices justified and explained to them; they wanted to be educated about the value and relevance of procedures; they noticed when prices were not competitive; and they were angered when they felt unnecessary treatments were being prescribed. When these needs were met, however, cost became simply 1 element among many in the mix. As 1 patient wrote, "It is very expensive; however, you get excellent and high-quality treatment." Another said, "Yes, everything could be very expensive, but you are now better able to make an informed decision on the work you want, or for financial or other reasons, do not want to perform."
Thus, Quebec dentists should take comfort from the fact that their patients have many positive things to say about what they are doing right; and learning from the negative comments will further strengthen patient care. The online forum is only one way to gather this information, however; more proactive approaches could include soliciting commentary by providing an anonymous patient feedback box in the dental office or hiring a graduate student to conduct a patient satisfaction survey of current and past clients, to determine what is working well and what could be improved.
Limitations
This research drew on information in a public online forum; thus, the strengths and limitations inherent in such a forum are limiting factors in our study. For example, it is impossible to know how representative this data set is. Further, although only 1 comment is allowed per IP address, thereby limiting false claims, there is no way to confirm whether a user is actually a patient. Yet, studies are increasingly confirming the value of online rating data in understanding quality in primary care22 and are showing a positive correlation between online ratings and physician quality.16 Future research on online ratings is needed to determine how these surveys affect patient referrals, the reputation of the professionals being rated and patients' perceptions of quality of care.14,16
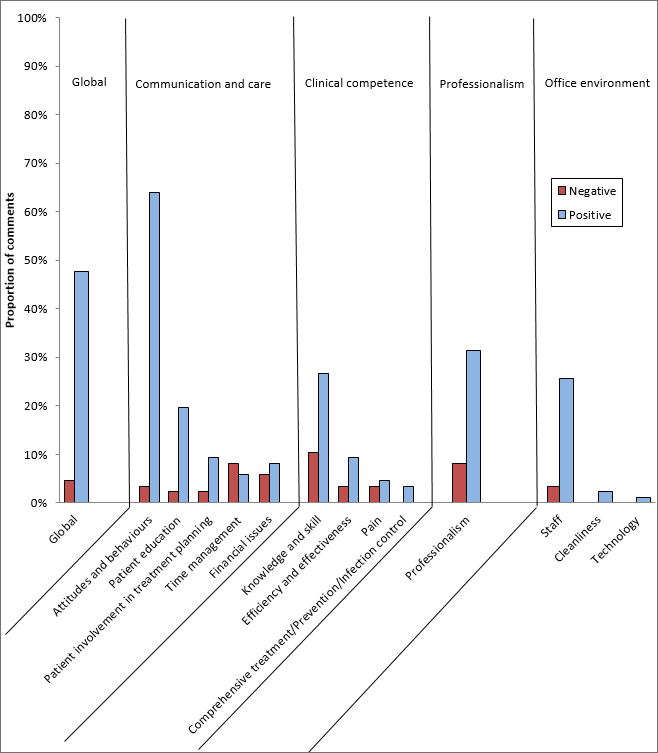 Figure 1: Abundance of comments by theme, subtheme and positive versus negative valence.
Figure 1: Abundance of comments by theme, subtheme and positive versus negative valence.
Conclusion
Our results suggest that patients in Quebec view their dentists very positively. Our findings reinforce the importance of patient-centred communication and care: patients seek dentists who respect them, care for them and educate them. Our data support ongoing communication skills training for dental students and dental teams, as well as continuing dental education.
THE AUTHORS
 |
Dr. Macdonald is assistant professor, division of oral health and society, faculty of dentistry, McGill University, Montreal, Quebec. |
 |
Ms. Beaudin is a DMD student, faculty of dentistry, McGill University, Montreal, Quebec. |
 |
Ms. Pineda is a research assistant, division of oral health and society, Faculty of Dentistry, McGill University, Montreal, Quebec. |
Acknowledgements
ME Macdonald was supported through a Chercheur-Boursier (Junior 1) salary award from the Fonds de recherche du Québec; A Beaudin was supported by a Summer Research Studentship from the McGill Faculty of Dentistry.
We would like to acknowledge Dr. Meredith Young and her team — ME Young, RL Cruess, SR Cruess and YS Steinert — for their contribution to the design of this project, especially through their research: Is a good clinical teacher seen as a good teacher by students and a good clinician by patients? (a poster presentation at the Research in Medical Education Conference, San Francisco, California, November 2012) and Do students and patients agree? Is a good clinical teacher seen as a good teacher and a good clinician? (an oral research presentation at the Canadian Conference for Medical Education, Banff, Alberta, April 2012).
Correspondence to: Dr. Mary Ellen Macdonald, Division of Oral Health and Society, Faculty of Dentistry, McGill University, #530-2001 McGill College Ave, Montreal, QC H3A 1G1. Email: mary.macdonald@mcgill.ca
References
- Duberstein P, Meldrum S, Fiscella K, Shields CG, Epstein RM. Influences on patients' ratings of physicians: physicians demographics and personality. Patient Educ Couns. 2007;65:270-4.
- Sbaraini A, Carter SM, Evans RW, Blinkhorn A. Experiences of dental care: what do patients value? BMC Health Serv Res. 2012;12:177.
- Reimann S, Strech D. The representation of patient experience and satisfaction in physician rating sites. A criteria-based analysis of English- and German-language sites. BMC Health Serv Res. 2010;10:332.
- Murray H, Locker D, Mock D, Tenenbaum H. Patient satisfaction with a consultation at a cranio-facial pain unit. Community Dent Health. 1997;14:69-73.
- Franks P, Fiscella K, Shields CG, Meldrum SC, Duberstein P, Jerant AF, et al. Are patients' ratings of their physicians related to health outcomes? Ann Fam Med. 2005;3:229-34.
- Silverman J, Kurtz S, Draper J. Skills for communicating with patients. 2nd ed. Oxford, UK: Radcliffe Publishing; 2005.
- Ipsos MORI. 2012 Annual patient and public survey: research report prepared for the General Dental Council: General Dental Coucil, London UK; 2012.
- Schouten BC, Eijkman MA, Hoogstraten J. Dentists' and patients' communicative behaviour and their satisfaction with the dental encounter. Community Dent Health. 2003;20:11-5.
- Hanley KJ. Counteracting an unflattering portrayal of dentistry. NY State Dent J. 2012;78:4-6.
- Croutze R. A tale of two realities. J Can Dent Assoc. 2010;76:a170.
- Gold SA. Cost of putting patients first: $0; professional credibility: priceless. J Calif Dent Assoc. 2008;36:537-8.
- Kuehn BM. More than one-third of US individuals use the Internet to self-diagnose. JAMA. 2013;309:756-7.
- Buchanan H, Coulson NS. Accessing dental anxiety online support groups: an exploratory qualitative study of motives and experiences. Patient Educ Couns. 2007;66:263-9.
- Black EW, Thompson LA, Saliba H, Dawson K, Black NM. An analysis of healthcare providers' online ratings. Informatics in Primary Care 2009;17:249-53.
- Lagu T, Hannon NS, Rothberg MB, Lindenauer PK. Patients' evaluations of health care providers in the era of social networking: an analysis of physician-rating websites. J Gen Intern Med. 2010;25:942-6.
- Gao GG, McCullough JS, Agarwal R, Jha AK. A changing landscape of physician quality reporting: analysis of patients' online ratings of their physicians over a 5-year period. J Med Internet Res. 2012;14:e38.
- Bacon N. Will doctor rating sites improve standards of care? Yes. BMJ. 2009;338:b1030.
- Hardey M. Consuming professions: user-review websites and health services. J Consumer Culture. 2010;10:129-49.
- Bell RA, Hu X, Orrange SE, Kravitz RL. Lingering questions and doubts: online information-seeking of support forum members following their medical visits. Patient Educ Couns. 2011;85:525-8.
- Fox S. The social life of health information. Washington, DC: Pew Research Center's Internet & American Life Project; 2011.
- Kadry B, Chu LF, Kadry B, Gammas D, Macario A. Analysis of 4999 online physician ratings indicates that most patients give physicians a favorable rating. J Med Internet Res. 2011;13:e95.
- Greaves F, Pape UJ, Lee H, Smith DM, Darzi A, Majeed A, et al. Patients' ratings of family physician practices on the internet: usage and associations with conventional measures of quality in the English National Health Service. J Med Internet Res. 2012;14:e146.
- Strauss A, Corbin J. Basics of qualitative research: techniques and procedures for developing grounded theory. 2nd ed. Newbury Park: Sage Publications; 1998.
- Statistiques : fiche sur la profession de dentiste au Québec. Montréal : Order des dentists du Québec; 2011. [accessed 2013 May 27] Available: http://www.odq.qc.ca/Publications/Statistiques/tabid/290/language/fr-CA/Default.aspx.
- Dentists. Ottawa: Government of Canada; 2011. [accessed 2013 May 27] Available: http://www.servicecanada.gc.ca/eng/qc/job_futures/statistics/3113.shtml .
- López A, Detz A, Ratanawongsa N, Sarkar U. What patients say about their doctors online: a qualitative content analysis. J Gen Intern Med. 2012;27:685-92.
- General Dental Council. Patient and registrant survey results. GDC Gazette 2011;Winter:10-1.
- Mead N, Bower P. Patient-centred consultations and outcomes in primary care: a review of the literature. Patient Educ Couns. 2002;48:51-61.
- Stewart M, Brown JB, Donner A, McWhinney IR, Oates J, Weston WW, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49:796-804.
- Abrahamsson KH, Hakeberg M, Stenman J, Öhrn K. Dental beliefs: evaluation of the Swedish version of the revised Dental Beliefs Survey in different patient groups and in a non-clinical student sample. Eur J Oral Sci. 2006;114:209-15.
- Rouse RA, Hamilton MA. Dentists' technical competence, communication, and personality as predictors of dental patient anxiety. J Behav Med. 1990;13:307-19.
- Abrahamsson KH, Berggren U, Hallberg L, Carlsson SG. Dental phobic patients' view of dental anxiety and experiences in dental care: a qualitative study. Scand J Caring Sci. 2002;16:188-96.
- Dong M, Levine A, Loignon C, Bedos C. Chinese immigrants' dental care pathways in Montreal, Canada. J Can Dent Assoc. 2011;77:b131.
- Loignon C, Allison P, Landry A, Richard L, Brodeur JM, Bedos C. Providing humanistic care: dentists' experiences in deprived areas. J Dent Res. 2010;89:991-5.
- MacEntee MI, Mariño R, Wong S, Kiyak A, Minichiello V, Chi I, et al. Discussions on oral health care among elderly Chinese immigrants in Melbourne and Vancouver. Gerodontology 2012;29:e822-32.