
ABSTRACT
Objective: To evaluate the translucency of currently available composites classified by their respective manufacturers as “opaque,” “dentin,” “body” (or “universal”) and “enamel” materials.
Materials and Methods: Four disk-shaped specimens were produced using a split-ring mould (13 mm in diameter and 2 mm in thickness) from each of 39 proprietary composite restorative materials. Enamel and dentin samples of equivalent thickness were obtained from extracted human teeth. Colour values for lightness (L*), red–green chromatic coordinate (a*) and blue–yellow chromatic coordinate (b*) were recorded against standard white and black backgrounds with a Minolta CR-300 chroma meter under the standard illuminant D65. Translucency parameter values were calculated and compared using analysis of variance and the Tukey test, with significance set at p < 0.05.
Results: A continuum of values for the translucency parameter was obtained, ranging from the most opaque (Filtek Supreme Plus A2D) to the most translucent (Ceram X Duo E2). In general, “opaque” and “dentin” composites yielded relatively low translucency values, “body” (or “universal”) composites yielded intermediate values, and “enamel” composites yielded relatively high values. However, the boundaries between these categories were not distinct, and there was some overlap. The mean value of the translucency parameter for human enamel was within the range of values for “enamel” shade composites. The individual values for specimens of human dentin were more variable (i.e., greater standard deviation around the mean) than those for human enamel. The mean value obtained for dentin was intermediate between the ranges for composites with low and intermediate translucency.
Conclusions: The various categories of composite from different manufacturers yielded a wide range of translucency, with minimal distinction between the extremes in adjacent categories. The measured translucency values provided more information than the respective category types. Knowledge of the relative translucency and opacity of different commercial materials can assist clinicians in the choice of composite for clinical use.
Introduction
Esthetic restorations require that the shade, shape and contour characteristics of the restoration be matched to those of the adjacent teeth. To render a restoration imperceptible, appropriate levels of translucency are also required. This characteristic can be idealized by harmonizing the optical properties of the restoration with those of the adjacent natural teeth. Composite resins tend to produce natural-looking restorations largely because they are relatively translucent. They provide a “chameleon” effect in small restorations, allowing the adjacent and underlying tooth structure to reflect or show through the restoration.1 For larger and more significant restorations, composite materials are available in a wide range of shades and opacities to allow duplication of adjacent tooth structure and enhancement of esthetic capabilities. Various levels of translucency have been developed to allow replication of the combined optical properties of dentin and enamel. More opaque composites can also be used to assist in masking the structure of discoloured teeth before the application of a more enamel-like translucent composite. A particularly challenging clinical situation involves Class III and IV restorations, which have no backing tooth structure. Without an appropriate level of dentinal opacity, even the most ideal shade of composite may appear too grey, because the relatively translucent composite is unable to mask the dark background of the oral cavity.2 Clinicians have devised “layering” techniques in which more translucent materials are placed over a more opaque composite in an effort to create depth from within the restoration.3
Several manufacturers now offer expanding lines of “enamel,” “dentin” and/or “body” (also known as “universal”) shade categories with differing levels of opacity and translucency. However, there is no standardization of the optical properties for these categories, and the results may be unexpected or disappointing. Recognition that the level of translucency of resin composites is a critical property, comparable in importance to the shade of the composite, has led many researchers to measure the translucency of specific resin composites in terms of the contrast ratio or translucency parameter.1-5 It is certainly advantageous for clinicians to know the translucency of a specific composite relative to that of the natural tooth structure. For many straightforward smaller restorations, the use of a shade-matched composite with intermediate opacity is simple and yields adequate results. However, in more critical esthetic situations, it may be necessary to layer several composites with different translucency and opacity properties to generate optimal, tooth-like esthetics. Information on the relative translucency and opacity of various composites is also useful in predicting the ability of proprietary composites to block out discoloured tooth structure or dark backgrounds.
The purpose of this study was to evaluate the translucency of currently available composites classified by their respective manufacturers as “opaque,” “dentin,” “body” (or “universal”) and “enamel” materials in relation to that of human enamel and dentin.
Materials and Methods
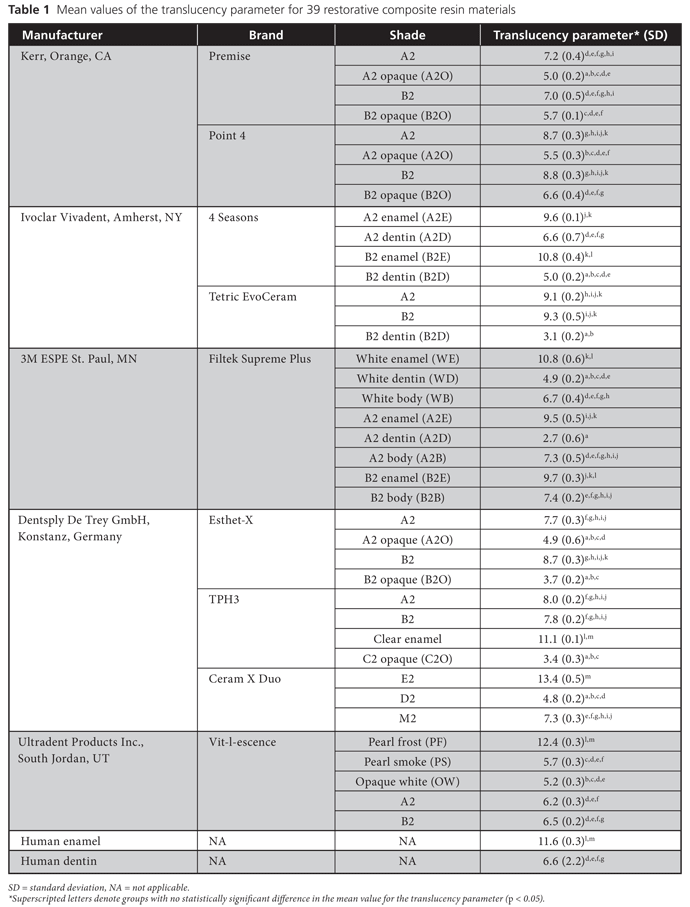
A total of 39 proprietary composite restorative materials were examined in this study (Table 1). Some manufacturers offer several subcategories of a brand, covering “enamel,” “body” (“universal”), “dentin” and/or “opaque” options. Wherever possible, 2 basic shades, A2 and B2, were tested for each category of opacity. Where this was not possible, the closest equivalent categories were tested.
Using a split-ring mould, 13 mm in diameter and 2 mm in thickness, 4 standardized disk-shaped specimens were prepared for each material. For each specimen, resin composite was introduced into the mould and pressed between 2 glass slides, with clear plastic film positioned between the composite and the glass. A weight was placed on the top slide for 2 minutes to produce uniform thickness. Light-curing was then applied for 40 seconds at each of 3 overlapping sites on both sides (i.e., 120 seconds on each side). The 2.0-mm thickness of the specimens was checked with a caliper to an accuracy of ± 0.1 mm. Samples of enamel (n = 3) and dentin (n = 6), also 2.0 ± 0.1 mm thick, were prepared by longitudinal sectioning of 3 extracted maxillary central incisors (for enamel) and 3 extracted permanent molars (for dentin), using a water-cooled low-speed diamond saw (Buehler Ltd., Lake Bluff, IL).
The specimens were stored in distilled water for 24 hours, after which they were blotted dry. The colour of each specimen was then measured, as follows. Values for L* (lightness, where 100 represents white and 0 represents black), a* (red–green chromatic coordinate) and b* (blue–yellow chromatic coordinate) were measured against a standard white background (L* = 89.33, a* = –5.27, b* = 7.41) and a standard black background (L* = 27.37, a* = –2.08, b* = 1.17) with a Minolta CR-300 chroma meter (Minolta Co. Ltd., Osaka, Japan), under the standard illuminant D65 (as defined by the International Commission on Illumination), which corresponds to “average” daylight. The measuring head of the chroma meter had an 8-mm diameter measuring area and used diffuse illumination and a viewing angle of 0°. The equipment was calibrated immediately before each set of measurements using calibration plate CR-A43, supplied by the manufacturer.
The translucency parameter was calculated as the difference in colour between the specimen as it appeared against the standard white background and as it appeared against the standard black background, according to the following equation:
TP = [(LW* – LB*)2 + (aW* – aB)*2 + (bW* – bB*)2]1/2
where W refers to the values for each specimen against the white background and B refers to the values for the specimen against the black background. Higher values for the translucency parameter represent greater translucency. The data were analyzed using analysis of variance (ANOVA) and Tukey’s tests, with significance set at p < 0.05.
Results
The mean values for the translucency parameter of these 2-mm thick specimens, with standard deviation (SD), ranged from 2.7 (SD 0.6) (most opaque) to 13.4 (SD 0.5) (most translucent) (Table 1).
Figure 1 shows the translucency parameter values in ascending order for all materials tested. The various categories of composite from the different manufacturers provided a wide range of translucencies, which formed a continuum from most opaque to most translucent. In general, the “opaque” and “dentin” composites had low translucency, the “universal” or “body” composites had intermediate translucency, and the “enamel” composites had high translucency (Fig. 1). However, the boundaries between these categories were not distinct, and some overlap occurred. No one manufacturer had products that were consistently most or least translucent across the various categories.
The composite with the lowest translucency (i.e., most opaque) was Filtek Supreme Plus A2D (“dentin” category), with a mean value of 2.7, and that with the highest translucency (i.e., most translucent) was Ceram X Duo E2 (“enamel” category), with a mean value of 13.4 (Table 1). The Filtek Supreme Plus A2D, Tetric EvoCeram B2D, TPH3 C2O and Esthet-X B2O specimens were significantly more opaque than specimens of human dentin. All of the “enamel” composites and 2 of the “body” or “universal” composites (Tetric EvoCeram A2 and B2) were significantly more translucent than dentin. Two “enamel” composites (Filtek Supreme Plus A2E and 4 Seasons A2E) were significantly less translucent than specimens of human enamel. Vit-l-escence A2 and B2 were the most opaque composites in the “body” or “universal” category. The Point 4 B2O and 4 Seasons A2D composites were more translucent than the “dentin” and “opaque” materials from other manufacturers and fell within the range of values for “body” rather than “opaque” composites.
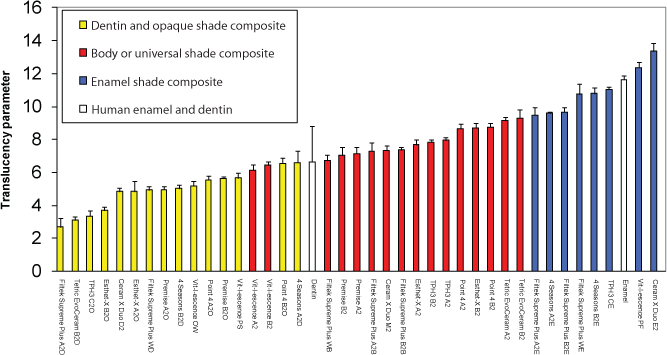 Figure 1: Mean translucency parameter values, with standard deviations, in ascending order, for all composite materials and categories tested. See Table 1 for definitions of abbreviated terms.
Figure 1: Mean translucency parameter values, with standard deviations, in ascending order, for all composite materials and categories tested. See Table 1 for definitions of abbreviated terms.
The mean translucency parameter for representative samples of tooth enamel (11.6 [SD 0.3]) was relatively high and fell within those obtained for composites in the “enamel” category. The translucency of the specimens of human dentin was more variable. The mean translucency parameter for the samples of tooth dentin (6.6 [SD 2.2]) was low to intermediate and fell between those obtained for the “dentin” and ”opaque” composites and those obtained for the “universal” or “body” composites.
Discussion
Translucency is the ability of a material to allow light to pass through and thus to allow the appearance of the underlying background to show through.6 It can be described as partial opacity or a state between complete opacity and complete transparency.5 The translucency parameter of a material refers to the difference in colour between a uniform thickness of the material over a white background and the same thickness of the material over a black background and provides a value corresponding to the common visual perception of translucency.7 A higher value for the translucency parameter represents greater translucency; if the material is completely opaque, the value of this parameter is zero.5,7 The translucency of tooth-coloured restorative materials is considered a crucial optical property, comparable in importance to colour,2,4 since the translucency will strongly affect the appearance of the same composite shade (Fig. 2). Knowledge of the relative translucency of proprietary composites can assist in the choice of product to achieve optimal esthetic results when attempting to either duplicate the optical properties of teeth or overcome the effects of discoloration or the dark background of the oral cavity.
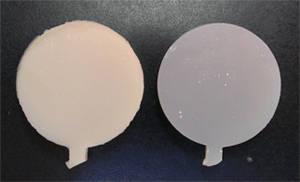 Figure 2: Composite specimens of the same shade on a standard black background, one with a low translucency parameter value (more opaque; on the left) and one with a high translucency parameter value (more translucent; on the right).
Figure 2: Composite specimens of the same shade on a standard black background, one with a low translucency parameter value (more opaque; on the left) and one with a high translucency parameter value (more translucent; on the right).
Although there have been several studies on the translucency of resin composites, only one has examined several different categories of composite from many manufacturers.5 The current study provides information on the relative translucency of 9 different brands of composite from 5 manufacturers for a total of 39 individual materials, focusing on 2 basic shades. The resulting range of translucency parameters for the 2-mm-thick specimens represents a continuum from most to least opaque (2.7 to 13.4). The most opaque group of composites, which had greater opacity than human dentin, could be used for masking darker background colours in the oral cavity using the layering technique.5 The majority of composites had translucency values within the wider range of values observed for human dentin. Within this group, the universal-shade composites varied from more opaque (Vit-l-escence A2 and B2) to more translucent (Tetric EvoCeram A2 and B2). There are therefore significant differences in light scattering, and hence translucency, among the so-called universal materials from different manufacturers, largely because of the specific composition and translucencies of the component materials, differences in the refractive index between filler and matrix, and differences in particle size.8 The less translucent composites are more likely to provide satisfactory results for the challenging Class III and IV restorations, which have no backing of tooth structure. The translucency values from this study provide the clinician with good comparative information on currently available proprietary materials. Caution is advised in extrapolating this information directly to all other shades of composite from the same manufacturer; however, there was a distinct trend for the 2 “universal” shades from each manufacturer that were tested (A2 and B2) to have similar translucency values.
Clinicians recognize that individual teeth will have greater or lesser translucency, and the relationship of translucency to age is well appreciated. Recently, an inverse relationship has also been shown between chroma (colour intensity) and translucency, which indicates that composites with high chroma are less translucent, and darker shades are less translucent.7 Translucency is significantly affected by polymerization, and the direction of change with polymerization (higher or lower) differs from one composite to another. Therefore, in cases where esthetics are critical, it is highly advisable to perform shade matching using polymerized composite.1,9,10 The materials in this study were all fully cured before testing.
Direct restoration with composite resins often provides the best, most conservative treatment option for replacement of tooth structure or enhancement of unesthetic teeth. Knowledge of the relative translucency of proprietary composites can assist in the choice of material and the achievement of optimal esthetics.
Conclusions
The various categories of composite (“enamel,” “body” or “universal,” “dentin,” “opaque”) from different manufacturers yielded a continuum of translucency values from most translucent to most opaque. Generally, the “opaque” and “dentin” composites had relatively low translucency, the “universal” or “body” composites had intermediate translucency, and the “enamel” composites had relatively high translucency. Because of the range of translucency values for different products within each category, the division between categories was indistinct. Therefore, the translucency values for specific products provide greater information than named category types. Information on the relative translucencies of commercial products can assist the clinician in choosing composites for clinical use.
THE AUTHORS
|
Dr. Ryan is a research associate in restorative dentistry, faculty of dentistry, University of Toronto, Toronto, Ontario. |
|
|
Dr. Tam is an associate professor in restorative dentistry, faculty of dentistry, University of Toronto, Toronto, Ontario. |
|
|
Dr. McComb is professor and head of restorative dentistry, faculty of dentistry, University of Toronto, Toronto, Ontario. |
Correspondence to: Dr. Dorothy McComb, Restorative dentistry, Room 352C, Faculty of dentistry, 124 Edward Street, Toronto, ON M5G 1G6.
Acknowledgements: The authors acknowledge donation of materials for the study from 3M ESPE and Dentsply Canada. The authors also thank Dr. Ralph W. Gilbert of the Wharton Head and Neck Centre, Princess Margaret Hospital, for loan of the chroma meter used in the study.
The authors have no declared financial interests in any company manufacturing the types of products mentioned in this article.
This article has been peer reviewed.
References
- Sidhu SK, Ikeda T, Omata Y, Fujita M, Sano H. Change of color and translucency by light curing in resin composites. Oper Dent. 2006;31(5):598-603.
- Ikeda T, Murata Y, Sano H. Translucency of opaque-shade resin composites. Am J Dent. 2004;17(2):127-30.
- Kim SJ, Son HH, Cho BH, Lee IB, Um CM. Translucency and masking ability of various opaque-shade composite resins. J Dent. 2009;37(2):102-7. Epub 2008 Nov 22.
- Ikeda T, Sidhu SK, Omata Y, Fujita M, Sano H. Color and translucency of opaque-shades and body-shades of resin composites. Eur J Oral Sci. 2005;113(2):170-3.
- Yu B, Lee YK. Translucency of varied brand and shade of resin composites. Am J Dent. 2008;21(4):229-32.
- Yu B, Ahn JS, Lee YK. Measurement of translucency of tooth enamel and dentin. Acta Odontol Scand. 2009;67:57-64.
- Yu B, Lee Y-K. Influence of color parameters of resin composites on their translucency. Dent Mater. 2008;24(9):1236-42. Epub 2008 Mar 28.
- Kim JJ, Moon HJ, Lim BS, Lee YK, Rhee SH, Yang HC. The effect of nanofiller on the opacity of experimental composites. J Biomed Mater Res B Appl Biomater. 2007;80(2):332-8.
- Woo ST, Yu B, Ahn JS, Lee YK. Comparison of translucency between indirect and direct resin composites. J Dent. 2008;36(8):637-42. Epub 2008 Jun 3.
- Lee YK, Powers JM. Color and optical properties of resin-based composites for bleached teeth after polymerization and accelerated aging. Am J Dent. 2001;14(6):349-54.