Abstract
Aim:
To evaluate level of compliance and reasons for non-compliance with measures to prevent dental injuries among ice hockey players.
Methods
Ice hockey players participated in an online, standardized, cross-sectional survey that addressed demographics, use and reasons for lack of use of facial and oral protective equipment and past oral injuries.
Results:
Of the 169 survey respondents, 45.6% never wore a mouthguard, 23.1% always, 14.8% sometimes and 16.5% only when enforced. Major reasons for not wearing mouthguards included discomfort, impairment of function or seeming unnecessary. Over 57.4% of participants wore a full-face shield, 35.5% a half-face visor and 7.1% no facial equipment. Participants did not wear a full-face shield mostly because it hinders visibility. Past oral injury was reported by 31.4% of participants. The most common type of injury was laceration (61.5%), followed by contusions, broken and lost teeth. Of the injured, 57.7% were hit by a stick, 46.2% by a puck and 25% were checked by an opponent.
Conclusions:
Compliance with wearing mouthguards and full-face shields is low because of issues surrounding player comfort, function and lack of visibility. Efforts should be made to work with hockey players and relevant industry to improve product design for protective measures and to enforce their use.
Practical Implications:
Reasons behind lack of protective equipment use by hockey players should be understood to enable dental professionals to communicate with patients and resolve challenges to the use of preventative measures to increase compliance and decrease incidence and severity of traumatic oral injuries.
Ice hockey is a popular sport internationally, with over 1 million players in Canada and the United States alone.1,2 This fast-paced collision sport has unique injury potential, as players can skate up to 30 mph and shoot pucks at over 100 mph with the constant risk of colliding into other players.3-5 The head and neck regions are considered particularly vulnerable to hockey-related injuries.6 Dental injuries have accounted for 11.5–16% of all ice-hockey-related injuries in previous reports.7,8 There are many known consequences of oral trauma, such as periapical lesions, pulp obliteration, loss of vitality, root resorption and tooth loss.9 Psychological and social impacts are also important, especially in children, as the consequences of dental trauma were shown to impair the social functioning, emotional balance and well-being of the child.10 A Finnish study11 showed that the most common dental trauma from ice hockey was a non-complicated crown fracture that occurred in 43.5% of all dental or maxillofacial injuries.
The incidence and type of facial injury is likely to depend on the type of facial protection worn by the player.3 The types of facial protection currently available include full-face shields, full-face cages, half-face visors and mouthguards. A prospective cohort study showed that the risk of dental injury for players wearing a half-face shield was 9.9 times higher than for those using a full-face shield.6 Additional studies have also concluded that the risk of dental injury is lowest with full-facial protection.3,7,12,13 Despite speculation that facial protection might increase the risk of concussions, studies show that full-face shields decrease concussion severity and rates of dental injuries without increasing the risk of other head injuries.12,14 Hockey Canada and USA Hockey mandate that all players wear helmets; however, full-facial protection for male players above the age of 18 is optional.15,16 Although some players choose to wear full-facial protection, others simply wear a half-face visor with a mouthguard. Nevertheless, a prospective study concluded that the combination of mouthguard and half-face shield does not provide sufficient protection against dental injuries.6 Ultimately, full-facial protection is necessary to decrease the risk of oral injury significantly.12
Studies have also shown that athletes are aware of injury risk, but still choose not to wear protective equipment.17 Moreover, players with a dental injury often present to an emergency room, where a dental professional is rarely available.18 The average cost of maxillofacial and dental injuries is over 3 times that of (non-dental) ice hockey injuries overall.7 Therefore, prevention of oral injuries would benefit player health as well as decrease the burden on the health care system. The aim of this study was to evaluate the level of compliance and reasons for non-compliance with regard to the use of preventive measures for dental injuries among ice hockey players and to assess the occurrence of past dental trauma.
Methods
An online cross-sectional survey was conducted among ice hockey players in Canada after the study was approved by the Research Ethics Board at the University of Alberta (Pro00075654). Data were collected between August 2017 and December 2019 through online distribution of questionnaires to current and past ice hockey players regardless of their experience with oral injuries. Each participant reviewed an information and consent form before answering the questions.
Questionnaires were completed online using a standardized form. The voluntary survey consisted of questions about participants’ demographics, use of facial protective equipment, reasons for not using protective measures, past oral injuries and opinion on the importance of such injuries in ice hockey. Quantitative data on demographics, level of compliance and past dental trauma were analyzed through cross-tabulation and descriptive statistics. Qualitative data on reasons for non-compliance were subjected to comprehensive inductive content analysis to interpret participant perspective. The levels of play indicated in the questionnaire were based on Hockey Canada’s stratification and descriptors.15
The survey included 15 multiple-choice questions and 6 short-answer questions, where participants could elaborate on their responses (Appendix A).
To participate in the study, players had to be over the age of 16 years (age of consent) when filling out the questionnaire and understand the consent form. Ice hockey associations from various jurisdictions were contacted with a description of the study and a link to the questionnaire. Participants were found at local ice-hockey games in Canada and we shared the link for the online survey. Players were encouraged to share this survey link with teammates. Regional ice hockey leagues were contacted with information about the survey and asked to share the link with its participants. The list of survey participants was reviewed to ensure there were no duplicate replies.
Results
Overall, 169 participants replied to the survey. Due to the nature of the distribution method we used for the surveys, we are unable to report on a response rate. Most of the participants were males (83.4%). The mean age was 30.04 ± 13.58 years (range 16–65 years). Most of the participants (67.5%) played at the Adult/Senior level, 22.5% at the Midget level and 10% at the Junior level. Participants who did not play co-ed hockey accounted for 69.3% of all survey replies. Of the participants, 12.1% had ≤ 10 years of experience, 49.7% had 10–20 years and 38.2% had > 20 years.
Mouthguard
Nearly half (45.6%) of the players never wore a mouthguard, 23.1% always, 14.8% sometimes and 16.5% only when it is enforced. Qualitative analysis of reasons for non-compliance revealed that many players found the mouthguard “uncomfortable,” “impairing function such as speaking, breathing, or drinking,” “inconvenient to play with,” “obtrusive,” “expensive,” “distracting,” “ill fitting,” “difficult to keep clean” and “inductive of a gag reflex.” Also, many participants reported that they did not think a mouthguard was really necessary (Table 1).
|
Theme |
Representative quotes |
|---|---|
| Comfort | “Annoying and uncomfortable” “Made me gag” “Hurts and bothers me when I play” “Very awkward thing” “Cumbersome and ill-fitting” |
| Necessity | “Unnecessary, I play pick-up hockey” “No one else uses it” “Don’t need one because I wear a cage” “Not required to use one by the league” |
| Function | “Inconvenient” “Can’t communicate” “Breathing and drinking is restricted” “Obtrusive and looks lame” “Difficult to keep clean” |
Face Shield
Over half (57.4%) of the participants wore a full-face shield, 35.5% a half-face visor and the rest wore no facial equipment while playing ice hockey. The inductive content analysis on non-compliance with facial equipment showed that most participants who do not use a full-face shield decide not to because it is “bulky to wear” and “hinders vision on the ice.” Most participants stated that if a full-face shield is not required by the league, they deemed it unnecessary to put up with the general discomfort. Players tended to prefer a half-face visor because it “offers better vision,” “fosters improved function” and “is perceived to have a better appearance” (Table 2).
|
Theme |
Representative quotes |
|---|---|
| Visibility | “Vision on ice is compromised” “Half-face visor easier to see through” “Wires from cage impede viewing ability” “Full-face shield fogs up” |
| Necessity | “Don’t need one because it’s restrictive” “Not mandated in my league” “No one else does so I don’t need to either” “I play shinny so not required” |
| Appearance | “Half-visor looks cooler” “Full-face shield too big and bulky” “Looks awkward because uncomfortable” |
Helmet
A few players (8.9%) reported never wearing an approved helmet properly. Instead, these players tended to adjust the chin cup/strap to avoid discomfort, minor cuts and difficulty communicating. In the short-answer section of the questionnaire, players reported not tying up the chin strap at all or tying it up improperly, so that it remains loose. One participant described wearing an expired helmet because a new one was too expensive (Table 3).
|
Theme |
Representative quotes |
|
|---|---|---|
| Sex (n = 1036) | ||
| Fit | “Doesn’t fit my face” “Too tight and restrictive” “Helmet doesn’t form to the shape of my face” “Chin-cup is annoying so I let it hang off my face” |
|
| Function | “Can’t talk” “Can’t breathe if straps are tight” “Chin-straps get in the way” “As visor fogs up I tilt helmet backwards” |
|
| Comfort | “Get cuts on my chin if I tie it up properly” “Straps, if tight, split my chin” “Using it properly is uncomfortable” “Chin-straps are uncomfortable, I don’t tie them up” |
|
Protective Equipment Compliance by Player Level
Midget players were the most compliant with the use of mouthguards, full-face shields and helmets (Table 4). After Midget players, Junior players had the best compliance with mouthguard use. However, Junior players had poorer compliance with use of full-face shields and helmets than Midget or Adult/Senior players.
|
Equipment |
Equipment |
|
||
|---|---|---|---|---|
|
Midget (n =38), % |
Junior (n =17),% |
Adult/Senior (n =114), % |
Total (n =169), % |
|
| Mouthguard | ||||
| Always | 37 | 18 | 20 | 23.1 |
| Sometimes | 16 | 29 | 12 | 14.8 |
| Only when enforced | 16 | 12 | 18 | 16.5 |
| Never | 31 | 41 | 50 | 45.6 |
| Facial equipment | ||||
| Half-face visor | 3 | 53 | 44 | 35.5 |
| Full-face shield | 97 | 35 | 47 | 57.4 |
| None | 0 | 12 | 9 | 7.1 |
| Helmet | ||||
| Always | 82 | 29 | 65 | 65.2 |
| Sometimes | 5 | 29 | 9 | 10 |
| Never | 13 | 42 | 26 | 24.8 |
Oral Trauma and Injury
In reviewing the occurrence of oral trauma, we found that 31.4% of participants reported an oral injury as a result of playing ice hockey. The most common type of injury was a laceration (61.5%) followed by contusions, broken teeth and lost teeth (Figure 1).
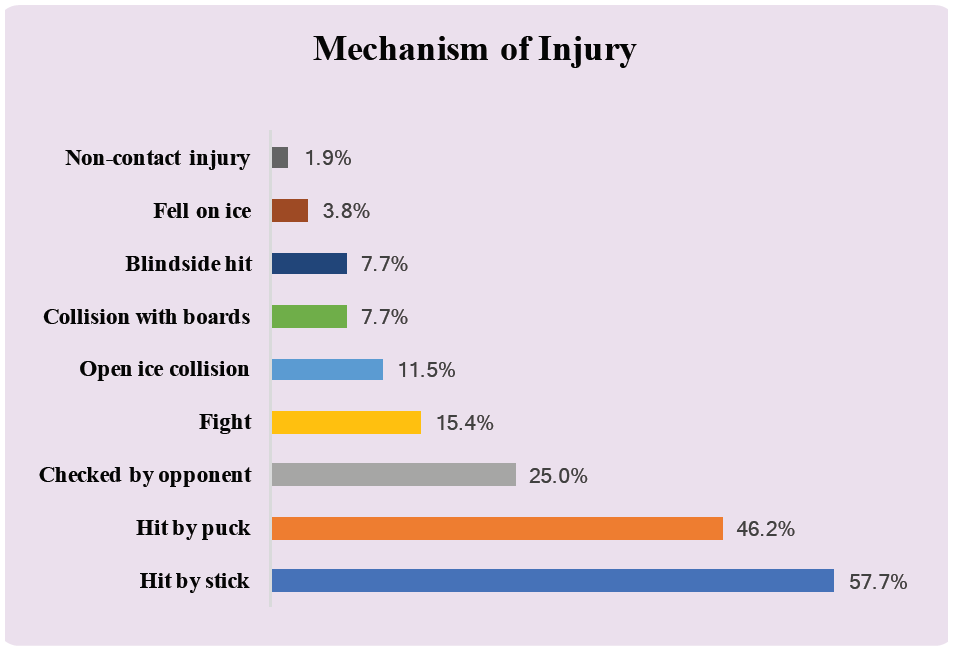
Figure 1: Classification of oral injuries as reported by survey participants (n = 169).
The age at injury ranged from 13 years* to 44 years, with a significant number of players having multiple injuries over the years. [*Note that 13 years refers to the age of the player at the time of the injury, not the age of the player when responding to the questionnaire. For example, a 25-year-old player could be reporting on an injury he had at age 13]. Among those injured, 66% had 1 or 2 injuries; the rest had 3 or more injuries (Figure 2).
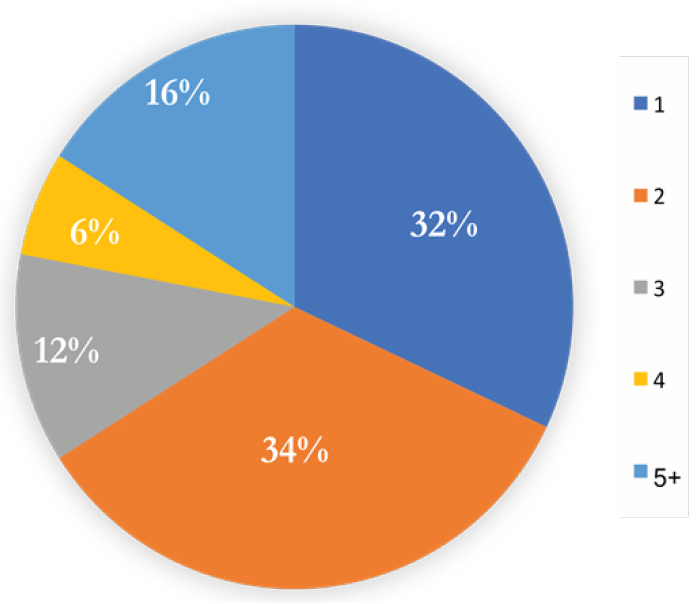
Figure 2: Number of oral injuries reported per player (n = 169).
Of the participants with past injuries, 23.5% missed playing time because of their injury. Of those injured, 49.0% were wearing a half-face visor when they were injured, while 19.6% reported not using facial protection at all at the time of injury.
Of those injured, 57.7% were hit by stick, 46.2% by puck and 25.0% were checked by an opponent (Figure 3).
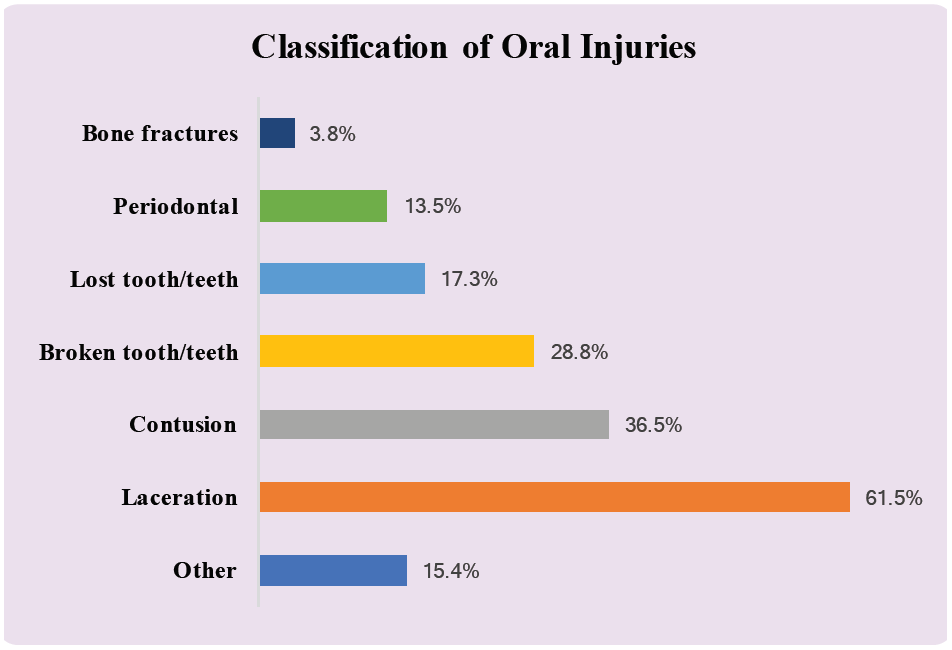
Figure 3: Mechanism of injury to ice hockey players (n = 169).
Treatment of injuries, as reported by the participants, included no treatment or follow-up, minor first aid, stitches, restorative procedures, extractions, root canal treatment, crown placement, surgery and others.
Opinion of Oral Injuries
Nearly half (45.8%) of participants believed that the issue of oral injuries is important, 45.2% believed that it is a small issue, while the remaining 9% did not think it is an issue at all.
Discussion
The nature of this survey allowed for collection of responses from a range of athletes, from those starting their careers in today’s age of player education about oral injuries to veteran players who have seen the sport change from no use of oral protective equipment to requiring full-facial protection for younger players.
According to our study, about a third of players suffer from oral injuries while playing ice hockey and most of these injuries are from being hit by a stick. This is consistent with other studies where 46.8% to 75.0% of oral injuries have resulted from a blow from a stick.5,6,11 Despite this, players prefer not to wear protective equipment for dental trauma for a variety of reasons.
According to our survey responses, the current level of compliance with wearing mouthguards is low because of issues with player comfort and function. Similar studies of mouthguard use by such athletes as rugby players and rowers have come to similar conclusions: general discomfort and difficulty in breathing or talking are chief reasons for dissatisfaction with mouthguards.19,20 In our study, players who did not wear a mouthguard recognized that they were at higher risk for dental injuries, but still chose not to wear one. Although the importance of mouthguard use to prevent oral injuries is well documented,8,17,19,21 players seem to believe that their comfort during the game outweighs any consequences. This should serve as a challenge to the dental community to educate players regarding the magnitude of the consequences of dental injuries.
Use of mouthguards is highest among Midget players and second highest among Juniors. This is understandable, as many regional leagues mandate mouthguard use at these levels, and non-compliance can lead to a penalty. However, it should be noted that mouthguard use is not universal. This could be a result of lack of enforcement of regulations by referees.
As oral health care providers, dental professionals can play a key role in preventing ice hockey players from sustaining dental injuries. They should educate patients about the importance of mouthguard use at regular dental visits. Starting a conversation about protective equipment might uncover the reasons for not using a mouthguard and allow dental professionals to highlight the consequences of not using such equipment. These include permanent tooth loss, unesthetic appearance and the potential need for extensive, expensive dental rehabilitation. By building a repertoire and arming themselves with evidence-based research, dental professionals may be able to convince patients to wear the appropriate protective equipment and, therefore, reduce the incidence of traumatic oral injuries.
Some survey respondents, who participate in pick-up hockey games (typically played with minimal equipment: skates, sticks and a puck or ball), reported that the laid-back atmosphere and lack of contact did not necessitate use of a mouthguard, especially as wearing one is not mandatory (Table 1). Dentists should emphasize that multiple studies, including the current one, demonstrate that the main causes of oral injury are a blow to the face by a stick or puck, which may occur during shinny. Although player contact might be lower during a pick-up game, players are still at risk of oral trauma.
Players may be more open to using a device that protects them from oral trauma if it is unobtrusive and more comfortable than a generic mouthguard; for example, a custom-made appliance. Patients should be informed that a randomized controlled trial showed that custom-made mouthguards have no detrimental effect on athlete performance.20 In fact, athletes regard custom-made mouthguards as comfortable and not causing breathing difficulty.20
Another approach to increase compliance might include education on the mechanism of action of a mouthguard in preventing oral trauma. A mouthguard acts as an impact-absorption device that dissipates the energy of a traumatic blow and serves as a cushion between the mandible and maxilla.22 If players better understood how a mouthguard protects them from injuries, they might be more inclined to use one.
Our study showed that use of full-face shields was lower than ideal because of visibility and comfort issues. Players preferred a half-face visor because, they claimed, it allows better vision, permits improved function (for drinking water, etc.) and looks better. Some participants felt that they were safe from dental injuries if they wear a mouthguard with their half-face visor. Dental professionals should explain to such players that wearing a mouthguard with a half-face visor is not enough to protect them from oral injury.6
Because a full-face shield is not required by every league, some players deem it unnecessary to put up with the additional bulkiness, obstruction of vision and general discomfort associated with this equipment, especially when their teammates choose not to wear full-facial protection. At the Midget level, 97% of players used a full-face shield, compared with 35% of Junior and 47% of Adult/Senior players. This could be attributed to a lack of enforcement or a difference in the culture surrounding use of protective equipment among the various leagues or both.
In addressing this issue, dental professionals should first empathize with the player and acknowledge the challenges associated with use of a full-face shield, but then emphasize the significantly lower occurrence of oral trauma with full- as opposed to half-face shields.3,6,7,12,13 A study that compared full-facial and half-visor protectors by striking them with pucks shot at high speeds (96–160 km/h) could also serve as an educational aid.23 This study showed that full-facial protectors did not permit any contact with the face until puck velocities exceeded 119 km/h, but half-visors resulted in facial contact for all visor impacts.23 This evidence leads to the conclusion that, although half-visors may protect from eye injury, they do not reduce the potential for serious facial lacerations or oral injuries.23 Such a discussion comparing the risks and benefits of half- versus full-face shields may be instrumental in convincing players to change their habits regarding use of protective equipment.
Another approach dental professionals may take is to advocate, on behalf of players, mandated use of full-face shields in all leagues for all players, regardless of age or gender. Studies show that boys report significantly higher levels of risk taking, more hostile, aggressive behaviour and lower levels of perceived risk than girls in team sports.24,25 In the past, rule changes have not addressed oral injuries to the same degree as other injuries, such as concussions.8 However, this seems to be changing with Hockey Canada’s recent ruling that mandates that all players below the Junior A level must wear full-facial protection.26 By collectively petitioning hockey authorities, dental professionals may be able to instill real change that could lead to a significant decrease in the incidence of oral trauma related to ice hockey injuries.
A case can be made for designing protective equipment that is more suitable and practical for players. These efforts should be made in consultation with hockey players and the relevant industry to optimize product design and to better enforce the use of such protective measures.
Some of the limitations of the current study are that the results are based on self-reporting and participant recall. Some players may have forgotten about injuries or neglected to report them, especially if they were minor. The data may also not completely reflect the occurrence of oral trauma in Canada because of selection bias in this convenience sample of participants. The study is only conclusive in the population observed, and confounding variables were not controlled for because of the observational nature of the study. In addition, self-reporting may have led to underreporting or exaggeration of oral trauma and level of compliance.
Conclusions
The current level of compliance with wearing mouthguards is low because of issues with player comfort and ability to function. Compliance with use of full-face shields is lower than ideal because of visibility and comfort problems. Efforts should be made to work with hockey players and the relevant industry to improve the design of protective equipment and to better enforce its use. This might, ultimately, increase compliance and decrease oral trauma.
THE AUTHORS
 |
Ms. Sarao is a DDS student, faculty of medicine and dentistry, University of Alberta. |
 |
Dr. Rattai is a private practitioner, Edmonton, Alberta. |
 |
Dr. Levin is a professor of periodontology in the faculty of medicine and dentistry, University of Alberta. He is also president-elect of the International Association of Dental Traumatology. |
Corresponding author: Prof. Liran Levin, University of Alberta, School of Dentistry, Faculty of Medicine & Dentistry, 5th floor, 5-468 Edmonton Clinic Health Academy, 1140 87 Ave NW, Edmonton AB T6G 1C9. E-mail: liran@ualberta.ca
The authors have no declared financial interests in any company manufacturing the types of products mentioned in this article.
This article has been peer reviewed.
References
- Hockey Canada annual report | July 2018 – June 2019. Ottawa: Hockey Canada; 2019. p. 15. Available: https://cdn.agilitycms.com/hockey-canada/Corporate/About/Downloads/2018-19-hockey-canada-annual-report-e.pdf (accessed 2020 May 8).
- 2018–2019 season final registration reports. Colorado Springs: USA Hockey; 2019. p. 3. Available: https://cdn1.sportngin.com/attachments/document/e36f-2180287/2018-19_Final_Registration_Report.pdf#_ga=2.37966112.2033110479.1621525433-1759106908.1621525420 (accessed 2020 May 8).
- Cohn RM, Alaia MJ, Strauss EJ, Feldman AF. Rink-side management of ice hockey related injuries to the face, neck, and chest. Bull Hosp Jt Dis. 2013;71(4):253-6.
- Mölsä J, Kujala U, Näsman O, Lehtipuu TP, Airaksinen O. Injury profile in ice hockey from the 1970s through the 1990s in Finland. Am J Sports Med. 2000;28(3):322-7.
- Deits J, Yard EE, Collins CL, Fields SK, Comstock RD. Patients with ice hockey injuries presenting to US emergency departments, 1990–2006. J Athl Train. 2010;45(5):467-74.
- Benson BW, Mohtadi NG, Rose MS, Meeuwisse WH. Head and neck injuries among ice hockey players wearing full face shields vs half face shields. JAMA. 1999;282(24):2328-32.
- Sane J, Ylipaavalniemi P, Leppänen H. Maxillofacial and dental ice hockey injuries. Med Sci Sports Exerc. 1988;20(2):202-7.
- Rattai J, Levin L. Oral injuries related to ice hockey in the province of Alberta, Canada: trends over the last 15 years. Dent Traumatol. 2018;34(2):107-13.
- Häyrinen-Immonen R, Sane J, Perkki K, Malmström M. A six-year follow-up study of sports-related dental injuries in children and adolescents. Endod Dent Traumatol. 1990;6(5):208-12.
- Lee JY, Divaris K. Hidden consequences of dental trauma: the social and psychological effects. Pediatr Dent. 2009;31(2):96-101.
- Lahti H, Sane J, Ylipaavalniemi P. Dental injuries in ice hockey games and training. Med Sci Sports Exerc. 2002;34(3):400-2.
- Asplund C, Bettcher S, Borchers J. Facial protection and head injuries in ice hockey: a systematic review. Br J Sports Med. 2009;43(13):993-9.
- Stuart MJ, Smith AM, Malo-Ortiguera SA, Fischer TL, Larson DR. A comparison of facial protection and the incidence of head, neck, and facial injuries in Junior A hockey players. A function of individual playing time. Am J Sports Med. 2002;30(1):39-44.
- LaPrade RF, Burnett QM, Zarzour R, Moss R. The effect of the mandatory use of face masks on facial lacerations and head and neck injuries in ice hockey. A prospective study. Am J Sports Med. 1995;23(6):773-5.
- Referee’s case book/rule combination 2018–2020. Ottawa: Hockey Canada; 2018. p. 38.
- Rule 304: protective equipment. In USA Hockey mobile rulebook. Colorado Springs: USA Hockey; 2020. Available: https://www.usahockeyrulebook.com/page/show/1084402-rule-304-protective-equipment (accessed 2020 May 8).
- ADA Council on Access, Prevention and Interprofessional Relations; ADA Council on Scientific Affairs. Using mouthguards to reduce the incidence and severity of sports-related oral injuries. J Am Dent Assoc. 2006;137(12):1712-20.
- Figueiredo R, Rattai J, Fournier K, Levin L. Emergency department visits for dental problems associated with trauma in Alberta: a report between the years 2011 and 2017. Dent Traumatol. 2018;34(6):421-8.
- Ilia E, Metcalfe K, Heffernan M. Prevalence of dental trauma and use of mouthguards in rugby union players. Aust Dent J. 2014;59(4):473-81.
- Duddy FA, Weissman J, Lee Sr RA, Paranjpe A, Johnson JD, Cohenca N. Influence of different types of mouthguards on strength and performance of collegiate athletes: a controlled-randomized trial. Dent Traumatol. 2012;28(4):263-7.
- Sekulic M, Kühl S, Connert T, Krastl G, Filippi A. Dental and jaw injuries sustained by hooligans. Dent Traumatol. 2015;31(6):477-81.
- Tuna EB, Ozel E. Factors affecting sports-related orofacial injuries and the importance of mouthguards. Sports Med. 2014;44(6):777-83.
- Smith T, Bishop P. Impact of full face and visor type hockey face guards. In: Safety in Ice Hockey. Castaldi C, Hoerner E, editors West Conshohocken, PA: ASTM International; 1989. p. 235-9.
- Kontos AP. Perceived risk, risk taking, estimation of ability and injury among adolescent sport participants. J Pediatr Psychol. 2004;29(6):447-55.
- Coulomb‐Cabagno G, Rascle O. Team sports players’ observed aggression as a function of gender, competitive level, and sport type. J Appl Soc Psychol. 2006;36(8):1980-2000. Available: https://doi.org/10.1111/j.0021-9029.2006.00090.x
- Kelloway B. Full-face protection now the ruled for 2 levels of N.S. junior hockey. Nova Scotia: CBC News; 2019. Available: https://www.cbc.ca/news/canada/nova-scotia/full-face-protection-shields-now-mandatory-junior-hockey-1.5232128 (accessed 2020 May 8).
Appendix A: Survey of ice hockey players
- What level of hockey do you play?
- Midget
- Junior
- Adult/Senior
- What is your age?
- What is your gender?
- Male
- Female
- Other
- Do you play co-ed hockey?
- Yes
- No
- How many years of ice hockey experience do you have?
- 0-2
- 2-4
- 4-6
- 6-8
- 8-10
- 10-12
- 12-14
- 14-16
- 16-18
- 18-20
- 20+
- Do you normally wear a mouthguard when playing hockey?
- Always
- Sometimes
- Only when enforced
- Never
- If you do not always wear a mouthguard, why not?
- What kind of facial protection do you wear on your helmet?
- Full-face shield
- Half-face visor
- None
- If you do not wear a full-face shield, why not?
Proper helmet wear clarification
From Hockey Canada’s rulebook15:
The chin-straps of the helmet shall be securely fastened under the chin. The straps of the facial protector, when designed to allow such straps, shall also be securely fastened to the hockey helmet.
In addition:
All straps should be properly tightened to a secure position. The chin cup is properly positioned comfortably against the chin. Vertical force clips positioned properly on the lateral aspects on the top of the cage/helmet. The helmet and face shield should be certified.
- Do you wear an approved helmet in the proper manner (see details above) when playing hockey?
- Always
- Sometimes
- Never
- If you do not always wear your helmet properly, why not? Please describe how you do wear it.
In the questions below, an oral injury is defined as any kind of injury to the oral (mouth) region affecting the teeth, gums, lips, bone, skin or tongue. A past injury does not have to have been significant, nor do you need to have missed playing time or received any kind of treatment. Please answer all the questions you can.
- Have you ever received an oral injury (dental, oral soft tissue or bone), however minor, before, as a result of playing ice hockey?
- Yes
- No
- What kind of oral injury? (select multiple if it applies)
- Soft tissue (lips, cheeks, tongue, skin)
- Dental (teeth)
- Bone
- How many oral injuries?
- 1
- 2
- 3
- 4
- 5+
- What category would you classify your injury (injuries) as? (select multiple if it applies)
- Lost tooth/teeth
- Broken tooth/teeth
- Contusion (bruise)
- Laceration (cut)
- Periodontal (gums)
- Fractured bone (broken upper/lower jaw)
- Other (describe below)
- Did you miss any playing time due to your injury?
- Yes
- No
- How old were you when you were injured?
- What kind of facial/oral protection were you wearing when you received your oral injury? (If you have multiple injuries and were wearing something different each time, indicate in the comment section. Select multiple options below if applicable.)
- Full-face shield
- Half-face visor
- Mouthguard
- No facial protection
- By what mechanism did your injury occur?
- Hit by stick
- Hit by puck
- Collision with boards
- Checked by opponent
- Open ice collision
- Fight
- Non-contact injury
- Collision with net
- Fell on ice
- Blindside hit
- Please describe the injury, how it occurred, the treatment received and any follow-up that was required.
- What is your attitude towards the issue of oral injuries in ice hockey?
- An important issue
- A small issue
- Not an issue