Abstract
Objectives:
To compare trends in teaching and placement of composite resin versus amalgam in posterior restorations in Canadian dental schools with those in the United States.
Methods
Secondary descriptive and statistical analyses were performed on data from 2 previous studies. The data consisted of responses to questionnaires on teaching policies and the proportion of posterior restorations (amalgam and composite resin) performed in Canadian and US dental schools. Fisher’s exact test and 2-sample z-test were used to compare the proportions.
Results:
Canadian dental schools allocated less time than US schools to teaching composite resin restorations (p = 0.006): 22.2% of Canadian schools versus 76.4% of US schools devoted more than 50% of preclinical teaching time to such restorations. Canadian dental schools also dedicated more time to teaching amalgam restorations (p = 0.041): 33.3% of Canadian schools versus 8.8% of US schools devoted 50–75% of preclinical teaching time to amalgam restorations. Between 2008 and 2018, a significantly higher proportion of composite resin restorations were performed in US dental schools than in Canadian schools (p < 0.001).
Conclusions:
In Canadian dental schools, teaching of posterior composite resin restorations was more conservative than in US schools. There was no consensus among Canadian and US dental schools on composite resin preparation techniques or contraindications. Clear, standardized guidelines pertaining to composite resin teaching policies are suggested.
Introduction
In the use of restorative material, a clear shift has occurred from dental amalgam to composite resin, representing a switch from the “extension for prevention” concept to a non-invasive or minimally invasive approach. Amalgam has been the material of choice for over 150 years because of its strength, durability, resistance to heavy occlusal load and effectiveness in challenging scenarios. However, its use in restorative dentistry has been reduced worldwide for many reasons. Apprehension about mercury in the population contributed to this trend, particularly after the Minamata Convention of 2013.1 In addition, preparing cavities for use of amalgam requires unnecessary removal of sound tooth structure to ensure sufficient resistance and retention, which can be avoided to an extent when using composite resin.2
Composite resins have become extremely popular over the years. Their esthetic properties and the advantage of conservative cavity preparation have made them preferred over other restorative materials.3 When directions for use are followed meticulously during placement, composite resins can exhibit excellent clinical performance.4,5 Thus, this has become the material of choice for restoring posterior cavities in private practice and dental schools worldwide.6-8 For instance, a 2021 survey among German dentists indicated that younger dentists frequently and increasingly offered composite resin restorations to their patients.9 In dental schools around the world the teaching of posterior composites has increased and surveys 10,11 have revealed institutions that have adopted an amalgam-free curriculum. At the same time, many schools still favour teaching amalgam placement.10
Our group recently investigated the latest teaching policies regarding the use of composite resin and amalgam in Canadian and United States (US) dental schools.10,11 We also determined the numbers of composite resin and amalgam posterior restorations placed in Canadian and US dental school clinics. In examining that data, we found a misalignment between the amount of time devoted to teaching each restorative material and the number of corresponding posterior restorations placed by students.10,11 Our investigation also revealed that in the US, the percentage of dental schools teaching posterior composite resin placement is higher than in Canada, and a higher percentage of dental schools mandate a competency test for class II composite restorations. In Canada, most schools teach amalgam placement techniques before composite resin placement, while fewer schools teach amalgam before composite resin in the US.10,11 On the other hand, Canadian dental schools are more comfortable teaching students to perform complex restorations using composite resin.10,11
Other teaching inconsistencies were also noted in both countries and are highlighted in the present study. An important factor to be considered is that graduates from Canada may practise dentistry in the US and vice versa. Thus, teaching and understanding the nuances surrounding different restorative techniques in both countries may raise North American dentists’ awareness of patients’ expectations and clinical decision-making. Hence, the objective of the current study was to compare policies on teaching placement of composite resin versus amalgam in Canadian and US dental schools; to compare the proportion of composite resin and amalgam restorations placed in Canadian and US dental schools over 10 years from 2008 to 2018; and to present general teaching trends in posterior restoration. The null hypotheses were: There are no differences in teaching policies between Canadian and US dental schools and There is no difference in the proportion of composite resin and amalgam posterior restorations being taught in Canadian and US dental schools.
Materials and Methods
Secondary descriptive and statistical analyses were performed on data from 2 previous studies.10,11 These data fall into 2 categories. The first are questionnaire responses received from Canadian and US dental schools.10,11 All responses were analyzed descriptively and using Fisher’s exact test to reveal differences. They include the following information: percentage of teaching time devoted to each type of restoration and the technique taught first (composite resin or amalgam) in preclinical teaching; competency tests conducted for each type of restoration in preclinical and clinical courses; contraindications considered and taught for each type of restoration; and features of cavity design taught for class II composite resin and amalgam preparations. In addition, the matrix system, light curing units and adhesive system used for bonding posterior composites, teaching techniques and resin materials used in Canadian and US dental schools were also assessed.
The second set of data included the number of posterior restorations of each type placed in Canadian and US dental schools.10,11 Secondary data analyses were performed descriptively and using a 2-sample z-test for proportions. Descriptive analysis was used to compare the proportions of composite resin and amalgam posterior restorations in dental schools of both countries. It also compares the turning point in each country, i.e., the year in which the number of composite restorations exceeded amalgam restorations. Also, annual growth rates among Canadian and US dental schools were compared. The 2-sample z-test for proportions was used to reveal in which country composite resin restorations were placed at higher numbers.
Statistical Analysis
Descriptive analysis was used to compare questionnaire responses; however, statistical analysis (Fisher’s exact test) was used to examine the differences between questionnaire responses. A level of significance of 5% was used for all inferential analyses, with p < 0.05 considered statistically significant.
In addition, descriptive analysis was used to compare the proportions of composite resin and amalgam posterior restorations in Canadian and US dental schools. A 2-sample z-test for proportions was performed for each year to assess when the proportion was significantly higher.
Data were organized in an Excel 2016 spreadsheet (Microsoft, Redmond, Wash., USA). Inferential statistical analyses were performed using SPSS v. 27 (IBM Corp., Armonk, NY, USA).
Ethics approval
The University of Toronto Research Ethics Board granted an exemption to the current study.
Results
Questionnaire Responses from Canadian and US Dental Schools
Preclinical Teaching of Posterior Restorations
In Canada, 78% of dental schools devoted 25–50% of their preclinical restorative teaching time to placement of composite resins (Table 1). In contrast, 76% of US dental schools devoted over 50% of time to posterior placement of resins. Looking to the future, 44% of Canadian dental schools reported that more time would be allocated to teaching composite resins; 41% of US dental schools predicted that more time would be assigned to the same subject. In regard to amalgam teaching, 56% of Canadian dental schools assigned 25–50% of their restorative teaching time to this technique, while 50% of US dental schools devoted ≤ 25% of teaching time. In the future, 11% of Canadian schools indicated that less time would be allocated to teaching amalgam in preclinical courses. At the same time, 44% of US schools anticipated less time spent on the same subject.10,11
|
Questionnaire |
US schools |
Canadian schools |
Fisher’s exact test, p |
|---|---|---|---|
| % time allocated to teaching posterior composite resins in preclinical courses | 0.006 | ||
| 25–50% | 8 (23.5%) | 7 (77.8%) | |
| 50–75% | 13 (38.2%) | 2 (22.2%) | |
| > 75% | 13 (38.2%) | 0 (0%) | |
| % time allocated to teaching amalgam in preclinical courses | 0.041 | ||
| < 25% | 17 (50.0%) | 1 (11.1%) | |
| 25-50% | 14 (41.2%) | 5 (55.6%) | |
| 50-75% | 3 (8.8%) | 3 (33.3%) | |
| Mandate for clinical competency test for class II composite resin | 0.024 | ||
| No | 1 (2.9%) | 3 (33.3%) | |
| Yes | 33 (97.1%) | 6 (66.7%) | |
| Teaching beveled gingival margin of proximal box technique for amalgam | 0.024 | ||
| No | 33 (97.1%) | 6 (66.7%) | |
| Yes | 1 (2.9%) | 3 (33.3%) |
Fisher’s exact test revealed that Canadian dental schools dedicated less time to teaching composite resin placement than their US counterparts (p = 0.006); 22.2% of Canadian schools versus 76.4% of US schools spent more than 50% of preclinical teaching on composite resin. Correspondingly, Canadian dental schools allocated more time to teaching amalgam than US dental schools (p = 0.041); 33.3% of Canadian schools versus 8.8% of US schools spent 50–75% of teaching time on amalgam (Table 1).
Competency Tests for Posterior Composite and Amalgam Restorations in Preclinical and Clinical Teaching
In preclinical courses, competency tests were indicated for class II restorations with both composite resin and amalgam equally in 89% of Canadian dental schools and 91% of US schools. In clinical courses, competency tests were indicated for composite resin and amalgam equally in 67% of Canadian dental schools, whereas in the US, tests for composite resin restorations were required in 97% of schools, compared with 53% for amalgam restorations.10,11 Fisher’s exact test showed that a significantly greater proportion of US schools mandated a clinical competency test for class II composite resin restorations compared with Canadian schools (97.1% vs. 66.7%, p = 0.024; Table 1).
Order of Teaching
Teaching amalgam placement techniques before composite resin techniques in preclinical courses was the practice in 89% of Canadian dental schools versus 62% of US dental schools.10,11 However, Fisher’s exact test showed that this difference was not significant (p > 0.05).
Contraindications for Posterior Placement of Composite Resin and Amalgam
We found no significant differences between Canadian and US dental schools in the teaching of contraindications to placement of composite resins (Table 2) and amalgams (Table 3).10,11
|
Contraindications |
% of respondent schools |
Fisher’s exact test, p |
|
|---|---|---|---|
|
Canada |
US (n = 34) |
||
| Poor oral hygiene/high caries risk | 89 | 56 | 0.121 |
| Cavity gingival margin on root surface | 56 | 41 | 0.477 |
| Inability to place a rubber dam | 89 | 71 | 0.407 |
| Parafunctional activity (bruxism) | 22 | 32 | 0.699 |
| Tooth acting as removable partial denture abutment | 33 | 41 | 1.00 |
|
Contraindications |
% of respondent schools |
Fisher’s exact test, p |
|
|---|---|---|---|
|
Canada |
US (n = 34) |
||
| Parafunctional activity (bruxism) | 11 | 12 | 1.00 |
| Tooth acting as removable partial denture abutment | 11 | 15 | 1.00 |
| Patient mercury concerns | 89 | 79 | 1.00 |
| Contact with dissimilar metal | 67 | 50 | 0.467 |
| Pregnant patient | 11 | 29 | 0.407 |
Cavity Design Features
In terms of cavity design, teaching of the use of composite resins (Table 4) or amalgams (Table 5) in Canadian and US schools was similar except for 1 feature.10,11 Fisher’s exact test showed a statistically significant difference (p = 0.024) in teaching beveling of the gingival margin of the proximal box in amalgam preparations between Canadian (33.3%) and US schools (2.9%).
|
Technique |
% of respondent schools |
Fisher’s exact test, p |
|
|---|---|---|---|
|
Canada |
US (n = 34) |
||
| Beveled occlusal margins | 11 | 18 | 1.00 |
| Beveled gingival margin of proximal box | 44 | 27 | 0.417 |
| Slot-type cavities (i.e., no occlusal component) | 89 | 85 | 1.00 |
| Reverse curve | 22 | 15 | 0.624 |
|
Technique |
% of respondent schools |
Fisher’s exact test, p |
|
|---|---|---|---|
|
Canada |
US (n = 34) |
||
| Beveled gingival margin of proximal box | 33 | 3 | 0.024 |
| Slot-type cavities (i.e., no occlusal component) | 22 | 35 | 0.693 |
| Retention grooves in full scale class II | 78 | 59 | 0.446 |
| Retention grooves in slot–type class II | 44 | 59 | 0.477 |
| Reverse curve | 89 | 79 | 1.00 |
Matrix Systems and Light Curing
All Canadian dental schools preferred to teach the “sectional matrix and separating ring” technique for class II composite resin restorations. Likewise, 97% of US schools chose to teach the same technique.10,11 In 78% of Canadian dental schools, LED curing is the system of choice in their faculty clinics when curing posterior composite resin restorations, compared with 97% of US dental schools that reported exact information.10,11 We found no significant differences between Canadian and US dental schools (p > 0.05).
Adhesive Systems and Composite Materials
In Canada, 56% of respondent schools taught students to use only the 3-step adhesive system (etch-prime-bond), and 44% of schools used the 2-step adhesive system only for bonding composite resin in posterior restorations. Although US dental schools taught variable types of systems, combined or alone, for bonding posterior composite resins, 56% taught students to use the 3-step adhesive system and 50% of schools used self-etching with selective etching. Moreover, 29% of surveyed US schools taught students to use self-etching (2-step system), and 24% used self-etching (1-step system) for posterior composite resin bonding.10,11 Fisher’s exact test showed no significant differences between Canadian and US dental schools (p > 0.05) in this regard.
Bulk-fill composite material was included in posterior restoration teaching in 44% of Canadian dental schools, compared with 41% of US schools. In Canada, 67% of surveyed schools indicated that they teach cusp build-up techniques using composite resins, compared with 56% of US schools.10,11 Fisher’s exact test revealed no significant differences between Canadian and US dental schools (p > 0.05).
Proportion of Composite Resin and Amalgam Restorations Performed in Canadian and US Dental Schools Clinics
We collected the numbers of posterior composite resin and amalgam restorations performed between 2008 and 2018 in most of the schools that participated in the study. In Canadian dental schools, there was an increase in the placement of posterior composite resin restorations over these years.10,11 However, composite resin was not used significantly more than amalgam until 2013.10,11 US dental schools also witnessed an increase in the placement of posterior composites resin restorations, and the number of these restorations became significantly greater than amalgam restorations in 2009.10,11
In Canadian dental schools, the proportion of posterior restorations performed using composite resin increased from 46% in 2008 to 69% in 2018, representing an average annual increase of 2.5%. That of restorations using amalgam decreased from 54% to 31% in the same period10,11 (Figure 1). In US dental schools, the proportion of composite resin restorations increased from 50% to 84% (an average annual increase of 3.7%), and that of amalgam restorations decreased from 50% to 16% in that period.10,11
A 2-sample z-test showed a significantly higher proportion of posterior restorations performed with composite resin in US schools than in Canadian schools each year from 2008 to 2018 (all p values < 0.001; Figure 1).
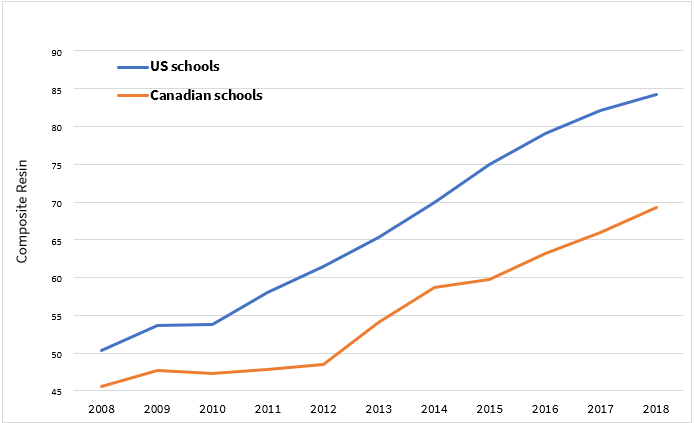
Figure 1: Proportion of posterior resin composite restorations performed in Canadian (n = 9) and United States (n = 34) dental schools.
Discussion
All of the 90% of Canadian and 52% of US dental schools that participated in this study are members of the American Dental Education Association (ADEA) and share a similar teaching system. However, their questionnaire responses revealed differences but also some similarities between the 2 countries. Therefore, our first null hypothesis was rejected.
The main significant difference between countries was in the time allocated to teaching composite resin and amalgam placement in preclinical courses, with Canadian dental schools dedicating less time to composite resin placement and more time to amalgam placement in preclinical courses compared with US schools (Table 1). This may explain the significantly higher proportion of posterior restorations performed using composite resin in US versus Canadian schools from 2008 to 2018.
In 2006, Lynch and colleagues12 showed that Canadian dental schools placed more composite resin (49% vs. 31%) and fewer amalgam restorations (51% vs. 62%) than US schools. However, those were estimates, not actual numbers. In dental schools in the United Kingdom, posterior composite resin placement techniques accounted for 36% of preclinical program in operative dentistry teaching time (range: 10–75%), and amalgam placement techniques accounted for 25% (range: 10–45%).13 In Austria, Germany and Switzerland, 76% of dental schools still teach amalgam placement, although it accounts for only 8% of the preclinical teaching.14 No information was reported about the time allocated to teaching composite resin placement.
Students who graduated in 2018 from North American dental schools are expected to practise dentistry for many decades. The procedures that novice students learn and the amount of training they receive during undergraduate years shape and influence their careers and clinical decision-making. As mentioned, most Canadian dental schools allocate up to 50% of their curriculum to amalgam teaching. However, in faculty clinics, students placed more composite resin in posterior teeth, nearly 70% of the total number of posterior restorations in 2018.10 These same students who received less instruction in composite resin placement will likely practise in a climate where this material is the first (and eventually only) treatment choice for most patients. Hence, schools and educators should ensure that dental students receive rigorous training to master the necessary procedures.
The other difference between Canadian and US dental schools was in competency tests mandated for class II composite resin restorations in clinics, with 97.1% of US schools versus 66.7% of Canadian schools mandating such a test (p = 0.024) (Table 1). A competency examination is an assessment tool that has a critical role in evaluating the efficiency of provided education and whether students have achieved the expected learning objectives. Berrong et al.15 investigated the effectiveness of a traditional daily grading system versus performance on 26 clinical competency tests where students would work without supervision. They concluded that competency tests provided a more reliable assessment of students’ capacity to perform core skills.
It was interesting to note that 89% of Canadian dental schools taught amalgam placement techniques before composite resin techniques in preclinical courses compared with 62% of US dental schools. In contrast, most dental schools in Japan and the United Kingdom have been teaching composite resin placement techniques before amalgam since 2005.16,17 Teaching resin techniques first allows dental students to base their approach to restorative dentistry on a preventive, minimally invasive treatment of caries rather than on invasive and mechanical retentive principles, to which students can transition gradually at a later stage.18
An additional difference between Canadian and US dental schools was in cavity design features. A larger proportion of Canadian schools (33.3%) taught students to bevel the gingival margin of the proximal box in class II amalgam preparations compared with US schools (2.9%, p = 0.024) (Table 1). Also, 89% of Canadian dental schools regarded “Poor oral hygiene/high caries risk” as a contraindication to placing composite resin in posterior teeth compared with 56% of US dental schools (Table 2), although the difference was not statistically significant. Based on these findings, there is no consensus on preparation techniques or contraindications for posterior restorations among North American dental schools.
Notably, the same percentage (56%) of Canadian and US dental schools taught their students to use the 3-step adhesive system (etch-prime-bond) when placing posterior composite resins. These adhesives have been available since the early 1990s and are considered the “gold standard” because this mode offers the highest immediate bonding strength. Nonetheless, after etching, demineralized dentin cannot be fully penetrated by resin, leaving some collagen fibers exposed. Thus, the bonding interface seems to be more susceptible to biodegradation.19-22 A systematic review and meta-analysis comparing the bond strength of universal adhesive using different etching modes found no significant difference between an etch-and-rinse and a self-etch mode in immediate or long-term bond strength, which indicates that the self-etch mode can achieve excellent bond strength.23
In addition, 44% of Canadian dental schools included bulk-fill composite material in teaching composite resin restorations compared with 41% of US schools. Placing bulk-fill material is less time-consuming and it can be polymerized adequately.24 A systematic review and meta-analysis demonstrated comparable clinical performances of bulk-fill and conventional composite resins over a follow-up period of 12–72 months.25
Of note, the percentage of Canadian dental schools (67%) that reported teaching cusp build-up techniques using composite resin was higher than the percentage of US dental schools (56%). This discrepancy between US and Canadian schools can be explained by a fear of a high risk of failure when placing resin composites in multi-surface and complex cavities. However, the clinical performance of composite resin restorations has been considered satisfactory and has improved over the past decades.26 A review and meta-analysis of treatment options for large posterior restorations found no significant difference in clinical performance between amalgam and composite resin.27 In addition, composite resin restorations can be more easily repaired, which may increase the longevity of a posterior restoration.28
Looking at the proportion of posterior restorations using composite resin or amalgam placed individually over 10 years from 2008 to 2018, we noted a significantly higher proportion of composite resin restorations among US schools compared with Canadian schools each year. In addition, Canadian dental schools used composite resins significantly more than amalgam for posterior restorations starting in 2013, while US schools started using composite resin more often in 2009. As our study did not explore determining factors, we can only speculate that these differences may be a result of factors such as differences in health care insurance systems or overall cultural differences and diversity between countries. Based on the noted differences, it is fair to state that Canadian dental schools have a more conservative approach to teaching composite resin restorations than US schools. As mentioned earlier, students who graduated in 2018 are expected to practise dentistry for several decades. Thus, teaching institutions should consider adapting their curriculum, taking into account evidence-based trends to better qualify dental professionals for future clinical practice.
One of the strengths of this study is the availability of data from 2 almost identical studies 10,11 (in the US and Canada) conducted by the same group, which made direct comparison possible in every aspect. Furthermore, this study was based on the first research to present North American trends in posterior restoration placement based on dental school numbers. On the other hand, this study did not compare posterior restorations using composite resin with other restorations, such as inlays and onlays. Not all dental schools teach undergraduate students to perform such restorations in clinics. Future studies should consider exploring and developing clearer guidelines for placing posterior composite resin restorations to aid the teaching curriculum.
Conclusion
Our comparison of Canadian and US dental schools demonstrated many differences and some similarities. The main difference was the amount of time allocated to teaching the use of composite resins for posterior restorations, with Canadian schools dedicating significantly less time to this subject than US schools. Also, students in Canadian schools placed significantly fewer posterior restorations using composite resin than in US schools each year from 2008 to 2018 . On the other hand, there was no consensus among Canadian and US schools on composite resin preparation techniques or contraindications. Therefore, clear, standardized guidelines pertaining to composite resin teaching should be discussed for all North American dental schools.
THE AUTHORS
 |
Dr. Al Reshaid is assistant professor, department of restorative and prosthetic dental sciences, College of Dentistry, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia, and assistant professor, King Abdullah International Medical Research Centre, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia. |
 |
Dr. El-Badrawy is emeritus professor, department of clinical Sciences, faculty of dentistry, University of Toronto, Toronto, Ontario, Canada. |
 |
Dr. Kulkarni is associate professor, department of pediatric dentistry, faculty of dentistry, University of Toronto, Toronto, Ontario, Canada. |
 |
Dr. Santos is associate professor, department of restorative dentistry, Schulich School of Medicine & Dentistry, University of Western Ontario, London, Ontario, Canada. |
 |
Dr. Prakki is professor, dental research institute, and associate dean, undergraduate education, faculty of dentistry, University of Toronto, Toronto, Ontario, Canada. |
Corresponding authors:
Dr. Lulwah Al Reshaid, P.O. Box 3660, Riyadh 11481, Saudi Arabia. Email: reshaidl@ksau-hs.edu.sa.
Dr. Anuradha Prakki, Room 547, 124 Edward St, Toronto ON M5G 1G6. Email: a.prakki@dentistry.utoronto.ca.
Acknowledgments: The Saudi Arabian Cultural Bureau supported this study with a grant to LA. The authors acknowledge the award of Dr. Miet and Mrs. Wanda Kamienski Professorship in Dental Education to AP.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Lynch CD, Wilson NHF. Managing the phase-down of amalgam: Part I. Educational and training issues. Br Dent J. 2013;215(3):109-13.
- Lynch CD. Successful posterior composites. London: Quintessence; 2008.
- Wong C, Blum IR, Louca C, Sparrius M, Wanyonyi K. A retrospective clinical study on the survival of posterior composite restorations in a primary care dental outreach setting over 11 years. J Dent. 2021;106:103586.
- Opdam NJ, van de Sande FH, Bronkhorst E, Cenci MS, Bottenberg P, Pallesen U, et al. Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. 2014;93(10):943-9.
- Pallesen U, van Dijken JW. A randomized controlled 27 years follow up of three resin composites in Class II restorations. J Dent. 2015;43(12):1547-58.
- Wilson NH, Lynch CD. The teaching of posterior resin composites: planning for the future based on 25 years of research. J Dent. 2014;42(5):503-16.
- Blum IR, Wilson NHF. An end to linings under posterior composites? J Am Dent Assoc. 2018;149(3):209-13.
- Eltahlah D, Lynch CD, Chadwick BL, Blum IR, Wilson NHF. An update on the reasons for placement and replacement of direct restorations. J Dent. 2018;72:1-7.
- Beyer C, Schwahn C, Meyer G, Söhnel A. What German dentists choose for their teeth: a web-based survey of molar restorations and their longevity. J Prosthet Dent. 2021;125(5):805-14.
- Alreshaid L, El-Badrawy W, Lawrence HP, Santos MJ, Prakki A. Composite versus amalgam restorations placed in Canadian dental schools. Oper Dent. 2021;46(6):621-30.
- Alreshaid L, El-Badrawy W, Kulkarni G, Santos MJ, Prakki A. Resin composite versus amalgam restorations placed in United States dental schools. Oper Dent. 2023;48(1):21-32.
- Lynch CD, McConnell RJ, Hannigan A, Wilson NHF. Teaching the use of resin composites in Canadian dental schools: how do current educational practices compare with North American trends? J Can Dent Assoc. 2006;72(4):321.
- Lynch CD, Blum IR, McConnell RJ, Frazier KB, Brunton PA, Wilson NHF. Teaching posterior resin composites in UK and Ireland dental schools: do current teaching programmes match the expectation of clinical practice arrangements? Br Dent J. 2018;224(12):967-72.
- Kanzow P, Büttcher AF, Wilson NHF, Lynch CD, Blum IR. Contemporary teaching of posterior composites at dental schools in Austria, Germany, and Switzerland. J Dent. 2020;96:103321.
- Berrong JM, Buchanan RN, Hendricson WD. Evaluation of practical clinical examinations. J Dent Educ. 1983;47(10):656-63.
- Lynch CD, McConnell RJ, Wilson NHF. Teaching of posterior composite resin restorations in undergraduate dental schools in Ireland and the United Kingdom. Eur J Dent Educ. 2006;10(1):38-43.
- Hayashi M, Seow LL, Lynch CD, Wilson NHF. Teaching of posterior composites in dental schools in Japan. J Oral Rehabil. 2009;36(4):292-8.
- Lynch CD, Frazier KB, McConnell RJ, Blum IR, Wilson NHF. Minimally invasive management of dental caries: contemporary teaching of posterior resin-based composite placement in U.S. and Canadian dental schools. J Am Dent Assoc. 2011;142(6):612-20.
- De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et al. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res. 2005;84(2):118-32.
- Hanabusa M, Mine A, Kuboki T, Momoi Y, Van Ende A, Van Meerbeek B, et al. Bonding effectiveness of a new ‘multi-mode’ adhesive to enamel and dentine. J Dent. 2012;40(6):475-84.
- Cardoso MV, de Almeida Neves A, Mine A, Coutinho E, Van Landuyt K, De Munck J, et al. Current aspects on bonding effectiveness and stability in adhesive dentistry. Aust Dent J. 2011;56 Suppl 1:31-44.
- De Munck J, Mine A, Poitevin A, Van Ende A, Cardoso MV, Van Landuyt KL, et al. Meta-analytical review of parameters involved in dentin bonding. J Dent Res. 2012;91(4):351-7.
- Chen H, Feng S, Jin Y, Hou Y, Zhu S. Comparison of bond strength of universal adhesives using different etching modes: a systematic review and meta-analysis. Dent Mater J. 2022;41(1):1-10.
- Hickey D, Sharif O, Janjua F, Brunton PA. Bulk dentine replacement versus incrementally placed resin composite: a randomised controlled clinical trial. J Dent. 2016;46:18-22.
- Veloso SRM, Lemos CAA, de Moraes SLD, do Egito Vasconcelos BC, Pellizzer EP, de Melo Monteiro GQ. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis. Clin Oral Investig. 2019;23(1):221-33.
- Alvanforoush N, Palamara J, Wong RH, Burrow MF. Comparison between published clinical success of direct resin composite restorations in vital posterior teeth in 1995–2005 and 2006–2016 periods. Aust Dent J. 2017;62(2):132-45.
- Vetromilla BM, Opdam NJ, Leida FL, Sarkis-Onofre R, Demarco FF, van der Loo MPJ, et al. Treatment options for large posterior restorations: a systematic review and network meta-analysis. J Am Dent Assoc. 2020;151(8):614-24.e18
- Loch C, Liaw Y, Metussin AP, Lynch CD, Wilson N, Blum IR, et al. The teaching of posterior composites: a survey of dental schools in Oceania. J Dent. 2019;84:36-43.