Abstract
Objectives:
The aims of this study were to characterize the type and frequency of oral and maxillofacial malignancies in an outpatient oral pathology service and to examine the impact of COVID-19 on the diagnosis of such malignancies by dentists in Ontario, Canada.
Study Design:
Our study included 775 malignancies submitted to an outpatient oral pathology service. Demographic and diagnostic data, including age, sex, submitting clinician type, anatomic site and diagnosis, were collected and analyzed for 2 periods, 2015–2019 and 2020.
Results:
Malignancies represented 2% of total submissions to our biopsy service. Oral surface epithelial malignancies were the most common, followed by hematologic and salivary gland malignancies. During the period in which dental offices were restricted (April–May 2020), 59% fewer malignancies were submitted compared with the preceding 5 years. Despite this reduction, total malignant submissions for 2020 and post-lockdown (July–September 2020) were significantly elevated compared with previous years (p = 0.0006 and p = 0.0008, respectively).
Conclusions:
Our study reaffirms the important role that dentists play in the diagnosis of oral and maxillofacial malignancies. Our assessment of 2020 data highlights the impact of dental office closures on the diagnosis of oral and maxillofacial malignancies during the COVID-19 pandemic.
Oral malignancies are uncommon, with previous studies reporting frequencies of 1.7–2.6% of all submissions to oral pathology biopsy services.1-5 Although rates as high as 5.4% have been reported in the United Kingdom (UK), geographic differences, as well as differences in referral patterns and population groups (hospital versus community) may partly explain this variability.1 Relatively few summative studies have focused on oral malignancies as a group, and, in Canada, such studies are rare.5 Dentists play an important role in the diagnosis of oral and maxillofacial malignancies. Examination of clinical data associated with malignancies provides important information about the types and frequency of lesions presenting in dental offices and provides an opportunity to observe changes in frequency patterns over time. A better understanding of the types of oral diseases affecting our populations will lead to the delivery of better oral health care.
The emergence of COVID-19, the illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and the subsequent effects on the provision of oral health care present a unique opportunity to examine the secondary effects of a global pandemic on the diagnosis of oral and maxillofacial malignancies, an area in which there exists a deficiency in the literature.6
Beginning in early 2020, the COVID-19 pandemic caused significant disruptions to the delivery of health care. In Ontario, the first known case of COVID-19 was identified on 25 January 2020. In early March 2020, case counts started to rise, leading to enhanced public health measures to mitigate spread of the disease. On 15 March 2020, Ontario’s Ministry of Health directed hospitals to ramp down non-emergent elective surgeries and clinical activities.7 On the same date, instructions strongly recommending suspension of all non-emergent care were issued to dentists by the Royal College of Dental Surgeons of Ontario,8 and, on 17 March 2020, the Government of Ontario declared a state of emergency, resulting in the lockdown of all non-essential services in the province. Full resumption of all non-urgent and elective care occurred on 26 May 2020, following a directive issued by the Ontario Ministry of Health.9
Because of shortages of personal protective equipment (PPE), many dental offices did not resume operations until mid-June 2020 or later. Tracking the re-opening of dental offices directly is difficult; however, data from the Canadian Dental Association over the pandemic period show that insurance claim volumes started to climb steadily in mid-June and reached 88% of 2019 claim frequency in Ontario by July 2020.10
Studies have shown that health care disruptions resulting from the COVID-19 pandemic have caused a decrease and, thus, ostensibly a delay in the diagnosis of many types of cancer; such trends have been reported in several locales, including the United States (US), Netherlands and the UK.11 Not surprisingly, the diagnosis of oral cancers has also been significantly affected by COVID-19 restrictions.12 Although the true impact of the COVID-19 pandemic on the diagnosis of oral and maxillofacial malignancies will not be known for several years, examining data trends before and after lockdown provides further insights.
The purpose of this study was twofold: to characterize the type and frequency of oral and maxillofacial malignancies submitted to an outpatient oral pathology service, and to examine the impact of the COVID-19 pandemic on the diagnosis of oral and maxillofacial malignancies by general dentists and dental specialists in Ontario, Canada. We hypothesize that the relative frequency of oral and maxillofacial malignancies is increased in 2020 relative to the last 5 years because of delays caused by COVID-19 pandemic related restrictions.
Methods
Demographic and diagnostic data were recorded for all biopsies with a malignant diagnosis submitted to the oral pathology diagnostic service (OPDS) at Western University, from 1 January 2015 to 30 September 2020. This included a small number of perioral skin malignancies. Clinical data included the patient’s age, sex, anatomic location of the biopsy, clinical diagnosis and histologic diagnosis. Information about the submitting clinician, including designation (specialist versus generalist) and specialist type, when appropriate, was also collected. Clinician category and specialty were determined using the public register available on the website of the Royal College of Dental Surgeons of Ontario. Clinical concordance was assessed using methods similar to those previously described by Patel et al.13 Cases were scored as concordant if the microscopic diagnosis and the clinical diagnosis were both suspected to be malignant. Cases were scored as discordant if the clinical diagnosis was suspected benign and the microscopic diagnosis was malignant. Cases submitted without a clinical diagnosis were excluded from this part of the analysis. Descriptive statistics were generated using SPSS v. 26.0 (IBM Corp., Armonk, N.Y., USA) and Prism v. 8.3 (GraphPad Software, San Diego, Calif., USA). Categorical data were analyzed using Χ2 or Fisher’s exact tests. Results were considered significant for p ≤ 0.05.
This study was approved by the Research Ethics Board at Western University, London, Ontario, Canada (REB no.114720).
Results
Number of Biopsies Submitted and the Impact of the COVID-19 Pandemic
The total number of biopsies submitted to OPDS between 1 January 2015 and 31 December 2019 was 33 212. The number of submissions to OPDS increased each year from 2015 to 2018, before dipping by 1% in 2019. In January 2020, submissions were nearly equal to those of 2019; in February, they were marginally elevated. However, in March they decreased dramatically, coincident with the closure of dental offices for non-emergent procedures commencing 17 March (Figure 1). Compared with the preceding 5 years, the number of biopsies was down 30% in March, followed by a record decline of 94% in April 2020. Beginning in May 2020, the number of biopsies began to increase, with the greatest increase noted in July, when total numbers were 88% of the previous 5-year average (Figure 1). By September, biopsy submission levels were 96% of 2015–2019 levels. Overall, biopsy submission levels in January–September 2020 were 31% below the previous 5 years.
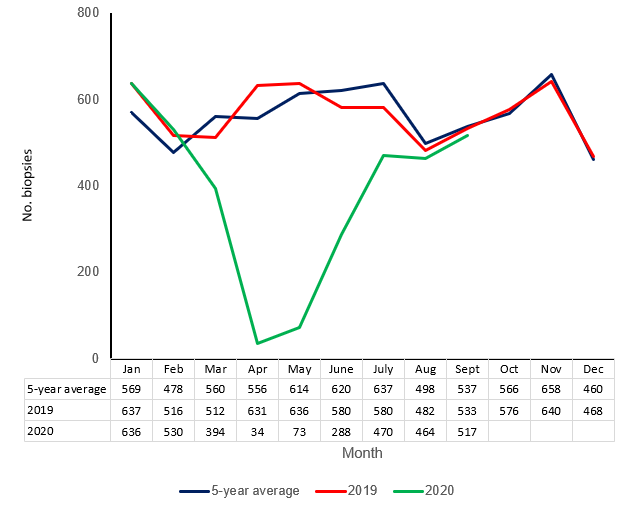
Figure 1: Total biopsy submissions by month for 2020 and 2019 and the 5-year average for 2015–2019.
Number of Malignancies Submitted and the Impact of the COVID-19 Pandemic
The total number of malignancies submitted to OPDS from 1 January 2015 to 31 December 2019 was 669, which represents an average relative frequency of 2%. Although the number of malignancies during this period increased for all years, except 2017, the increase was not significant.
In January–September 2020, 106 malignancies were submitted to OPDS. During the lockdown period (April–May 2020), 59% fewer malignancies were submitted to OPDS compared with the previous 5 years. Despite these reductions, total malignant submissions in 2020 (January–September inclusive) were significantly increased (p = 0.0006, Figure 2). Given the reopening timelines for dental offices in Ontario, the most pertinent data can be obtained from submissions during July–September 2020, as these months represented the period in which biopsy submission levels most closely approximated normal. The number of malignancies submitted over this period was significantly increased (p = 0.0008), with an average relative frequency of 3.9%, which represents a 1.8-fold increase over comparable periods in previous years (Figure 3).
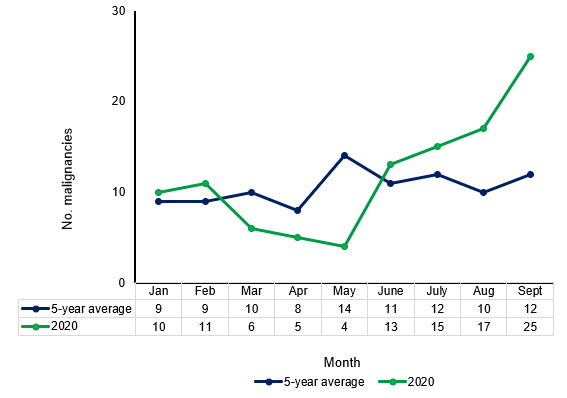
Figure 2: Total malignancies, by month, January–September, for 2020 compared with 5-year annual average for 2015–2019.
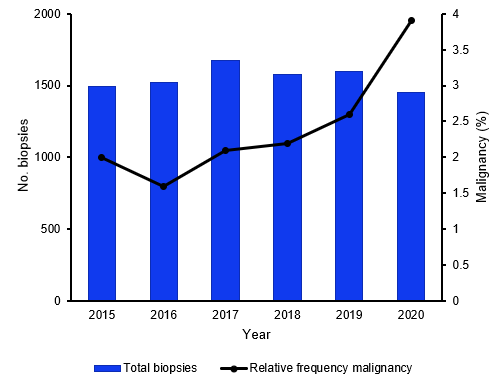
Figure 3: Relative frequency of malignancies and total biopsies by year, July–September.
Clinical Characteristics of all Submitted Malignancies (2015–2020)
During the study period, 775 malignancies were submitted to OPDS. The most common were surface mucosal epithelial malignancies (83.6%, oral squamous cell carcinoma and verrucous carcinoma, abbreviated hereafter as OSCC), followed by hematologic and salivary gland malignancies (7.1% and 4.4%, respectively), metastases (2.1%) and basal cell carcinomas (1.4%). Melanomas, sarcomas and odontogenic carcinomas were very uncommon, collectively representing 1.4% of all submitted malignancies (Table 1). The types of malignancies submitted during 2015–2019 and the 2020 period were similar, except for metastatic lesions. The frequency of metastases submitted in 2020 was notably higher than average yearly submissions for the preceding 5 years; however, this increase did not reach statistical significance (p = 0.0549).
|
|
2015–2019 |
Jan.–Sept. 2020 |
Total (2015-Sept. 2020) |
|---|---|---|---|
|
Note: SD = standard deviation. |
|||
| Total biopsies submitted | 33 212 | 3406 | 36 618 |
| Malignant biopsies | 669 | 106 | 775 |
| Relative frequency of malignancy, % | 2.0 | 3.1 | 2.1 |
| Age of patient, no. (%) | |||
| ≤ 45 years | 43 (6.4) | 9 (8.5) | 52 (6.7) |
| 46–60 years | 193 (28.8) | 27 (25.5) | 220 (28.4) |
| ≥ 61 years | 433 (64.7) | 70 (66.0) | 503 (64.9) |
| Mean age, years (SD) | 66 (13.9) | 66 (14.3) | 66 (14.0) |
| Sex, no. (%) | |||
| Male | 381 (57.0) | 46 (43.3) | 427 (55.1) |
| Female | 288 (43.0) | 60 (56.6) | 348 (44.9) |
| Type of malignancy, no. (%) | |||
| Surface epithelial | 560 (83.7) | 88 (83.0) | 648 (83.6) |
| Hematologic | 48 (7.2) | 7 (6.6) | 55 (7.1) |
| Salivary gland | 29 (4.3) | 5 (4.7) | 34 (4.4) |
| Metastatic | 11 (1.6) | 5 (4.7) | 16 (2.1) |
| Basal cell carcinoma | 10 (1.5) | 1 (0.9) | 11 (1.4) |
| Melanoma | 5 (0.7) | — | 5 (0.6) |
| Other* | 6 (0.9) | — | 6 (0.8) |
| Site, no. (%) | |||
| Lateral tongue | 167 (25.0) | 25 (23.6) | 192 (24.8) |
| Floor of the mouth | 112 (16.7) | 13 (12.3) | 125 (16.1) |
| Gingiva | 102 (15.2) | 24 (22.6) | 126 (16.3) |
| Buccal mucosa | 68 (10.2) | 15 (14.2) | 83 (10.7) |
| Other† | 220 (32.8) | 29 (27.3) | 249 (32.1) |
Age
Oral and maxillofacial malignancies most commonly affect people in the 7th decade of life, closely followed by those in the 8th and 6th decades. No substantial differences were found between the mean ages of patients during 2015–2019 and the 2020 period. Oral surface epithelial malignancies and salivary gland tumours showed a peak incidence among people in the 7th decade, whereas the peak incidence for hematologic malignancies was in the 8th decade. Of all submitted malignancies, the youngest mean age was associated with sarcomas (37.8 years, SD 23.8, range 18–66 years), while the oldest mean age was associated with melanomas (72 years, SD 12.1, range 55–86 years).
Sex
Overall, malignancies were more common in males (55.1%) than females (44.9%). However, during the 2020 period, more malignant submissions were received from female patients (Table 1). When subdivided by specific diagnosis, a male predominance was found in all malignant subgroups, except for salivary gland carcinomas and melanomas (Table 2).
Anatomic Site
The site of occurrence was available for 773 of 775 cases. When all malignancies are considered, the most commonly affected site was the lateral tongue (24.8%), followed by the gingiva (16.3%) and the floor of mouth (16.2%). When non-OSCC malignancies are examined, the most commonly affected sites included the palate for both hematologic (32.7%) and salivary gland cancers (52.9%) and the gingiva for metastases (56.3%, Table 2). All salivary gland carcinomas submitted to OPDS during the study period were from the minor salivary glands.
Most Common Diagnoses, by Malignant Sub-group
The most frequently diagnosed hematologic malignancy during the study period was diffuse large B-cell lymphoma (38.2%), followed by plasma cell neoplasms (14.5%), follicular lymphomas (12.7%) and lymphomas of mucosa-associated lymphoid tissue (12.7%, Table 2). The most common diagnoses for salivary gland malignancies, in order of decreasing frequency were: mucoepidermoid carcinoma (47.1%), adenoid cystic carcinoma (20.6%) and polymorphous adenocarcinoma (14.7%). The site of primary malignancy for the metastatic lesions was highly variable, and, notably, in 4 cases (25%), the tissue of origin could not be determined. When the tissue of origin was known, renal cell carcinoma of the kidney was the most common type of metastatic cancer (18.8%), followed by lung, liver and breast metastases (2 cases each, or 12.5%).
|
|
No. |
Age, years (SD) |
Sex |
Site, no. (%) |
Sub-classification, no. (%) |
|
|---|---|---|---|---|---|---|
|
Male |
Female |
|||||
|
Note: AdCC = adenoid cystic carcinoma, BM = buccal mucosa, DLBCL = diffuse large B-cell lymphoma, FL = follicular lymphoma, FOM = floor of mouth, MALT = lymphoma of mucosa-associated lymphoid tissue, MEC = mucoepidermoid carcinoma, OSCC = oral squamous cell carcinoma, PAC = polymorphous adenocarcinoma, SCC = squamous cell carcinoma, SLL/CLL = small cell lymphocytic lymphoma/chronic lymphocytic leukemia, UK = unknown, VC = verrucous carcinoma. *Site was not provided for 2 OSCC submissions. For OSCC, other sites include: lip (n=43), palate (n=31), oropharynx (n=15), jaws (n=50), retromolar pad (n=20), skin (n=2), missing (n=2). For hematologic malignancies, other sites include: FOM (n=1), lip (n=2), oropharynx (n=1), buccal mucosa (n=9), retromolar pad (n=1). For salivary gland malignancies, other sites include: FOM (n=2), jaws (n=3), lip (n=2). For metastases, other sites include: FOM (n=1), tongue (n=1). |
||||||
| OSCC | 648 | 66.2 (13.6) | 378 | 270 | Tongue: 190 (29.3) FOM: 121 (18.7) Gingiva: 106 (16.4) BM: 68 (10.5) Other*: 163 (25.2) |
SCC: 615 (94.9) VC: 33 (5.1) |
| Hematologic malignancies | 55 | 68.6 (13.3) | 33 | 22 | Palate: 18 (32.7) Jaws: 12 (21.8) Gingiva: 11 (20.0) Other*: 14 (25.5) |
DLBCL: 21 (38.2) Plasma cell: 8 (14.5) FL: 7 (12.7) MALT: 7 (12.7) SLL/CLL: 5 (9.1) Other: 7 (12.7) |
| Salivary gland malignancies | 34 | 57.4 (17.2) | 8 | 26 | Palate: 17 (50.0) BM: 5 (14.7) Retromolar: 5 (14.7) Other*: 7 (20.6) |
MEC: 16 (47.1) AdCC: 7 (20.6) PAC: 6 (17.6) Other: 5 (14.7) |
| Metastases | 16 | 63 (9.3) | 9 | 7 | Gingiva: 9 (56.3) Jaws: 5 (31.3) Other*: 2 (12.5) |
UK: 4 (25) Kidney: 3 (18.8) Breast: 2 (12.5) Liver: 2 (12.5) Lung: 2 (12.5) Other: 3 (18.8) |
Clinician Characteristics
The overwhelming majority of malignant biopsies submitted to OPDS during the study period were by dental specialists (97%), with oral and maxillofacial surgeons submitting 90.2%. Periodontists made up the next largest group, at 4.8%.
Clinical Diagnosis
Clinical impressions were measured by comparing the submitted clinical diagnosis with the final microscopic diagnosis. In 17 cases, no clinical diagnosis was submitted, and these cases were excluded from this part of the analysis. Clinical impressions were concordant with microscopic diagnosis in 84.5% of cases. There were no significant differences in the rates of concordance for diagnoses made during 2015–2019 and the 2020 period. Discordances were most common in the case of odontogenic malignancies at 100% (2/2), melanomas at 60% (3/5), metastases at 28.6% (4/14), salivary gland carcinomas at 26.5% (9/34) and sarcomas at 25% (1/4). Discordances were least common in oral surface epithelial malignancies (OSCC) at 11.3% (72/637) and basal cell carcinomas of the skin at 10% (1/10). In cases of hematologic cancer, 21% (11/52) of cases were discordant. As the number of malignancies submitted to our service by general dentists is small, it is unlikely that true differences between specialists and generalists can be assessed. However, based on our limited data, the rate of concordance for general dentists was lower than for specialists (76.2%).
Discussion
The relative frequency of malignancies submitted to our biopsy service (2%) is consistent with previously reported studies.4,5 Despite an increase in the total number of biopsies submitted to our service over the past 5 years, the relative frequency of malignancies has remained markedly stable. In 2020 (January–September, inclusive), the relative frequency of malignant submissions was significantly elevated compared with previous years (Figure 2).
Separating our data into 2 periods, lockdown and post-lockdown, provides further clarity about the significance of our findings. Given the restrictions placed on dental offices in Ontario from mid-March to May 2020 and the resultant decrease in total submissions to our service (94% decrease in April and 88% decrease in May), it is not surprising that the number of malignancies submitted during this time is also reduced compared with the last 5 years. As a result of this overall decline, malignancies make up a greater percentage of total submissions, resulting in a hugely elevated relative frequency, which peaked at 14.7% in April. Post-lockdown, as dental offices re-opened, overall biopsy submission levels began to increase, and the relative frequency of malignancies declined, as expected. However, it remained persistently and significantly elevated compared with the past 5 years. This persistent elevation provides further and more direct evidence that the diagnosis of a proportion of malignancies was delayed or missed during the lockdown period, and our data are consistent with those that have emerged from other countries suggesting that the diagnosis of oral cancer by dentists was depressed during the first wave of the COVID-19 pandemic.12,14
Delays in the diagnosis of oral cancer have been shown to be related to advanced tumour stage and a poor prognosis.15 Although the full impact on patient morbidity and mortality of diagnostic delays resulting from the COVID-19 pandemic will not be measurable for several years, recent modeling data suggest that the effects may be significant. A recent study from the UK16 examined the potential impact of diagnostic delays on cancer survival through stages I–III (i.e., patients who would be treated with curative intent) among the 20 most common human cancers. For oral cancer, Sud and colleagues16 extrapolate a resultant 10 year reduction in net survival of 12.83–18.28% or an estimated 190 additional lives lost attributable to a 6-month delay. Although frequency of cancer varies geographically, survival rates are similar in many economically developed countries, which allows for some generalizability of this model to other jurisdictions. Consideration of data like these is important for guiding future public health decisions, including the allocation of resources for clearing diagnostic backlogs in the face of ongoing waves of COVID-19 or future pandemics.16
The ability of dental practitioners to keep their offices open with sufficient PPE to deliver oral health care services safely is only one of many possible factors encountered during a pandemic that may impact the diagnosis of oral diseases. Patient-directed deferral in accessing an oral health care assessment is another potentially significant factor that can lead to delays in diagnosis, and subsequent increases in patient mortality. Most oral malignancies affect patients in the 7th decade of life, the age at which the risk of clinically significant COVID-19 infection and death start to increase.17 Patients may choose not to access appropriate health care services because of fear of contracting COVID-19 or because of age-specific government recommendations, and cases of delayed diagnosis of oral cancer as a result of patient decisions have been reported.18 During these uncertain times, a clear message that oral health care can be delivered safely, with appropriate COVID-19 precautions, such as patient and dental staff screening for COVID-19 symptoms and exposure, limiting non-urgent aerosolized procedures, increased office cleaning and appropriate social distancing measures, is imperative.
In many respects, our collated frequency data are similar to those reported in a recent study by Abadeh et al.5 Oral surface epithelial malignancies represent 1.8% of total submissions to our service and 83.6% of malignant submissions. Hematologic malignancies, with a frequency of 7.1%, represent the second most common type of malignancy in our data set, followed closely by salivary gland tumours at 4.4%. Although there is some variation in the relative incidence of the 3 most common types of oral malignancies in the literature, the small differences between our data and those of Abadeh et al., can be explained by the slightly higher incidence of OSCC in our malignant group (84% vs. 77%). There appears to be a small difference in the number of hematologic malignancies encountered in our study and those of Abadeh et al.5 when compared with others in the US (5.4%) and UK (5.9%),1,4 which may suggest that a higher relative frequency of hematologic malignancies exists in our population group.
Although the increase in the number of metastatic lesions over our study period was not itself significant, their number is likely to continue to increase because of delays in diagnosis and treatment caused by COVID-19. A recent study examining the effects of the COVID-19 pandemic on cancer diagnosis and treatment encounters in the US found that screening for breast and colorectal cancers fell dramatically from February to April 2020 compared with 2019 levels. This decrease in screening, coupled with a corresponding decrease in diagnoses, suggests the potential for more patients to present at later disease stages.19 The number of metastatic lesions submitted to our service, post-lockdown in 2020, was notably increased, with 4 out of 5 metastatic lesions diagnosed after dental care restrictions were lifted at the end of May 2020. Although it is too soon to draw any conclusions, this departure from the 5-year trend suggests that dentists may already be seeing the impact of diagnostic and treatment delays for systemic cancers. Further examination of changes in staging data over the coming years will be the most accurate and informative way to determine whether delays associated with the COVID-19 pandemic have resulted in later-stage disease at diagnosis.
Discordances between clinical and microscopic diagnoses are difficult to measure accurately and likely vary depending on type of lesion as well as the training and experience of the submitting clinician. Although the concordance rate between clinical and microscopic diagnoses in our study is higher than that in comparable studies,13 it is clear from our results that a substantial proportion of oral and maxillofacial malignancies cannot be predicted from clinical examination alone. This finding is not novel or surprising, as it is well known that some oral and maxillofacial malignancies can mimic benign or reactive oral lesions. The presentation of soft tissue metastases to the oral cavity is a well cited example of this phenomenon.20 However, given the expansion of teledentistry since the emergence of COVID 19, we believe this topic has particular relevance.
Teledentistry allows continuity of dental care by virtual means, whether by asynchronous assessment of photographs or in real time by video conferencing. Teledentistry has become an important and useful tool for preliminary patient assessments, particularly when restrictions are placed on in-person dental visits or for patients who may need to access dental care, but are required to quarantine. Teledentistry can also enable better access to care in underserviced communities. Before the emergence of COVID-19, teledentistry was not permitted in Ontario, and it is unclear currently how many dentists may be using teledentistry routinely for the assessment of oral lesions. Although a strong case can be made for the continued use of teledentistry to help clear patient backlogs created by pandemic-associated lockdowns and to facilitate care in instances where in-person visits are restricted, it is crucially important that dentists remain aware of the potential limitations of teledentistry, particularly as they relate to the assessment of oral pathologic lesions. Poor image quality, suboptimal lighting and dexterity limitations in patients retracting their own tissues, for example, could complicate diagnostic assessment and lead to misdiagnosis. In addition, the inability to accurately capture the texture of a lesion during a virtual assessment, a characteristic that depends on palpation, is also problematic.21
Our study has limitations. Our data are limited to a single diagnostic service, and data trends encountered in our service, although similar to those in another Canadian study5, have limited generalizability. The period of data collection for our study post-lockdown (3 months) was short; however, this period also reflected the time during which COVID-19 cases in Ontario were lowest. Although there have been no recent restrictive changes in the practice of dentistry in Ontario, the rapidly increasing daily case counts at the end of 2020 and into 2021 have necessitated increased public health measures directed at decreasing community spread, which may impact the number of patients seeking in-person dental care.
Conclusion
Our study reaffirms the important role of dentists in the diagnosis of various types of oral and maxillofacial malignancies. Further, our assessment of 2020 data highlights the impact of dental office closures on the diagnosis of such malignancies during the COVID-19 pandemic. We believe that these data will be useful in measuring the secondary effects of the global COVID-19 pandemic on the diagnosis of clinically significant oral diseases.
THE AUTHORS
 |
Ms. Juneja is a 4th year dental student, department of dentistry, Schulich School of Medicine and Dentistry, Western University, London, Ontario. |
 |
Mr. Aggarwal is a 3rd year dental student, department of dentistry, Schulich School of Medicine and Dentistry, Western University, London, Ontario. |
 |
Dr. McCord is an assistant professor, departments of pathology and laboratory medicine and dentistry, Schulich School of Medicine and Dentistry, Western University, London, Ontario; and a staff oral pathologist, departments of pathology and laboratory medicine and dentistry, London Health Sciences Centre, London, Ontario. |
Corresponding author: Dr. Christina McCord, Division of Oral Pathology, Department of Pathology and Laboratory Medicine, Western University, HSA 418A, 1151 Richmond St, London, ON N6A 4C1. Email: cmccord4@uwo.ca
This study was funded by the Schulich Dentistry Research Opportunity Program.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Jones AV, Franklin CD. An analysis of oral and maxillofacial pathology found in adults over a 30-year period. J Oral Pathol Med. 2006;35(7):392-401.
- Bhaskar SN. Oral pathology in the dental office: survey of 20,575 biopsy specimens. J Am Dent Assoc. 1968;76(4):761-6.
- Thompson CC. A six year regional report on the oral tumor registry and lesions diagnosed in the School of Dentistry Biopsy Service University of Oregon Health Sciences Center (Portland, Oregon). J Oral Med. 1981;36(1):11-5.
- Dovigi EA, Kwok EYL, Eversole LR, Dovigi AJ. A retrospective study of 51,781 adult oral and maxillofacial biopsies. J Am Dent Assoc. 2016;147(3):170-6.
- Abadeh A, Ali AA, Bradley G, Magalhaes MA. Increase in detection of oral cancer and precursor lesions by dentists: evidence from an oral and maxillofacial pathology service. J Am Dent Assoc. 2019;150(6):531-9.
- Shanti RM, Stoopler ET, Weinstein GS, Newman JG, Cannady SB, Rajasekaran K, et al. Considerations in the evaluation and management of oral potentially malignant disorders during the COVID-19 pandemic. Head Neck. 2020;42(7):1497-502.
- Ramping down elective surgeries and other non-emergent activities (memorandum to Ontario Health and hospitals). Toronto: Ministry of Health, Government of Ontario; 2020. Available: http://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/memos/DM_OH_CMOH_memo_COVID19_elective_surgery_March_15_2020.pdf (accessed 2020 Nov. 19).
- A message to all dentists in Ontario - COVID-19 pandemic. Toronto: Royal College of Dental Surgeons of Ontario; 2020. Available: https://www.rcdso.org/en-ca/rcdso-members/dispatch-magazine/articles/5286 (accessed 2020 Nov. 19).
- COVID-19 directive #2 for health care providers (regulated health professionals or persons who operate a group practice of regulated health professionals) issued under Section 77.7 of the Health Protection and Promotion Act (HPPA), R.S.O 1990, c. H.7. Toronto: Ontario Ministry of Health and Long-Term Care; 2020. Available: https://www.cdho.org/docs/default-source/pdfs/covid-19/directive-2-may-26-2020.pdf (accessed 2021 Aug. 30).
- By the numbers: business recovery from the pandemic. CDA Essentials. 2020;7(6):9-11. Available: http://www.cda-adc.ca/en/services/essentials/2020/issue6/8/ (accessed 2021 Aug. 30).
- Kaufman HW, Chen Z, Niles J, Fesko Y. Changes in the number of US patients with newly identified cancer before and during the coronavirus disease 2019 (COVID-19) pandemic. JAMA Netw Open. 2020;3(8):e2017267.
- Arduino PG, Conrotto D, Broccoletti R. The outbreak of Novel Coronavirus disease (COVID 19) caused a worrying delay in the diagnosis of oral cancer in north-west Italy: the Turin metropolitan area experience. Oral Dis. 2020;27 Suppl 3:742-3.
- Patel KJ, De Silva HL, Tong DC, Love RM. Concordance between clinical and histopathologic diagnoses of oral mucosal lesions. J Oral Maxillofac Surg. 2011;69(1):125-33.
- da Cunha AR, Antunes JLF, Martins MD, Petti S, Hugo FN. The impact of the COVID-19 pandemic on oral biopsies in the Brazilian National Health System. Oral Dis. 2020;10.1111/odi.13620. Online ahead of print.
- Gómez I, Seoane J, Varela-Centelles P, Diz P, Takkouche B. Is diagnostic delay related to advanced-stage oral cancer? A meta-analysis. Eur J Oral Sci. 2009;117(5):541-6.
- Sud A, Torr B, Jones ME, Broggio J, Scott S, Loveday C, et al. Effect of delays in the 2-week-wait cancer referral pathway during the COVID-19 pandemic on cancer survival in the UK: a modelling study. Lancet Oncol. 2020;21(8):1035-44.
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA. 2020;323(13):1239-42.
- Ianculovici C, Kaplan I, Kleinman S, Zadik Y. Guest editorial: COVID-19 and the risk of delayed diagnosis of oral cancer. Quintessence Int. 2020;51(10):785-6.
- London JW, Fazio-Eynullayeva E, Palchuk MB, Sankey P, McNair C. Effects of the COVID-19 pandemic on cancer-related patient encounters. JCO Clin Cancer Inform. 2020;4:657-65.
- Hirshberg A, Shnaiderman-Shapiro A, Kaplan I, Berger R. Metastatic tumours to the oral cavity — pathogenesis and analysis of 673 cases. Oral Oncol. 2008;44(8):743-52.
- Patel T, Wong J. The role of real-time interactive video consultations in dental practice during the recovery and restoration phase of the COVID-19 outbreak. Br Dent J. 2020;229(3):196-200.