Abstract
Background:
The onset of the COVID-19 pandemic and government restrictions affecting dental health care professionals had an impact on pediatric dental emergency trends. The purpose of this study was to describe the effect of the COVID-19 pandemic on the characteristics, outcomes and management of pediatric dental emergencies in a single tertiary care hospital.
Methods:
A retrospective review of children presenting to Montreal Children’s Hospital for dental emergencies before and during the pandemic was conducted. Data collected included children’s demographic characteristics, type of emergency visit, clinical signs and symptoms, as well as emergency management. For the pandemic period, data regarding patient symptoms of COVID-19 infection were also noted.
Results:
Of the 2745 pediatric dental emergencies included, 1336 (48.7%) occurred in 2019 and 1409 (51.3%) in 2020. During the first wave of COVID-19, the number of pediatric dental emergencies increased by 21% over pre-pandemic levels. A significant increase in the number of emergencies associated with dental infection was noted during the pandemic period (p = 0.04). A significant increase in the number of visits not receiving effective immediate treatment (p < 0.01) occurred during the early pandemic period.
Conclusions:
Our study shows a significant increase in the rates of dental emergencies and acuity of dental conditions during the first wave of the pandemic. Increased public health measures and adaptation to this ongoing public health crisis are important to ensure continued high-quality dental care for pediatric patients.
Introduction
The onset of the COVID-19 pandemic resulted in reduced access to dental care for the Canadian population1,2. Stay-at-home orders, curfews and lockdowns were enforced nationwide in an attempt to contain the virus.2,3 In March 2020, Quebec provincial governing bodies mandated that health care services be limited to emergencies.4 Consequently, elective dental care was deferred during the lockdown period. Guidelines outlining emergency criteria limited the number of patients who could present to their health care providers, including visits to designated tertiary care pediatric hospitals for dental emergencies.5
Similar large-scale public health measures were implemented by several countries to minimize the risk of viral transmission,6,7 affecting the provision of dental care on a global scale. Early indications suggest a substantial shift in patterns and trends of dental emergency admissions after the onset of the pandemic. In Italy, a country in which COVID-19 was notably prevalent, a significant decrease occurred in both pediatric and adult dental emergency admissions for both the lockdown and second-wave periods of the pandemic.8 A similar trend for the first wave was found in a Chinese study.9 In India, a decrease in the number of pediatric patients presenting for dental emergencies during the lockdown period was also observed.10 In contrast, an overall increase in daily volume of adult patients presenting for urgent dental care during the lockdown period was reported by a Swiss study.11
To date, few published data have characterized the effects of the pandemic on pediatric dental emergencies, especially those involving Canadian health care centres. A recent study from British Columbia12 described adult and pediatric dental emergencies during the first wave of the pandemic: dental trauma and odontogenic infections were the most common reasons for a visit, and the most frequent treatments were found to be consultations followed by oral surgical procedures. The purpose of this study was to determine the characteristics, outcomes and management of pediatric dental emergencies in a single tertiary care hospital during the pandemic period compared with the same time frame in 2019.
Methods
Research Design
This retrospective study was conducted at the Montreal Children’s Hospital (MCH), a tertiary care pediatric hospital that serves the greater Montreal area. The Division of Dentistry provides comprehensive primary and tertiary dental care for children, with an annual volume of approximately 22 000 visits. Emergency dental care is available 24/7 and is provided in-house by staff dentists and residents.
This study included all dental emergency visits during the first 2 waves of the COVID-19 pandemic (January to December 2020) and 1 year before the pandemic (January to December 2019). Although outside the lockdown period, January and February were included in the analysis to account for yearly variation in pediatric dental emergency volume, as well as to minimize seasonal differences. Patients less than 18 years of age who sought emergency dental care at the MCH during the study period were identified and included in the study. Confirmation of the first COVID-19 case in Canada occurred in January 2020. In March 2020, at the onset of the pandemic, restrictive policies had been established nationwide and access to pediatric dental care in Montreal was limited to only 2 pediatric hospitals. This study was approved by the ethics review board of the institution (2021-7514).
Data Collection
Patient visits were identified using billing codes in AD2.0 clinic management software (CLG Inc., Montreal, Canada). Dental records were reviewed for patient demographics, such as age and gender. Characteristics of the dental emergency visit, including diagnosis, type of visit (caries-related problems, traumatic dental injuries and others) and clinical signs and symptoms (presence of pain and presence of dental infection) were also collected. For the pandemic period, data regarding patient symptoms (i.e., fever, cough and headache) were noted. To ensure accuracy of data retrieved, 2 authors (MHB and MSM) reviewed all available information, and any discrepancies were resolved by consensus. Dental records with illegible and/or incomplete information were excluded from analysis.
Statistical Analysis
The data were subjected to descriptive analysis. Categorical variables were presented in terms of frequency and proportion; mean and standard deviation were calculated for continuous variables. A Χ2 test was used to compare variation in volume of pediatric dental emergencies before and during the pandemic. Analysis of differences in types of dental emergencies and emergency management for both periods were assessed using Fisher exact tests or Χ2 tests. A significance threshold of α = 0.05 was used for all analyses. All analyses were conducted using Statistical Package for Social Sciences (SPSS, v. 21.0).
Results
The analysis included 2745 pediatric dental emergencies. During the first year of the pandemic, a significant increase in the number of pediatric dental emergency visits occurred compared with the pre-pandemic period (1409 and 1336, respectively; 5.6% increase; p = 0.04). We noted no significant differences in children’s demographic characteristics between periods (Table 1). Significantly more pediatric dental emergencies associated with dental infection occurred during the pandemic period (p = 0.04).
|
Characteristic |
No. patients (%) |
|
|---|---|---|
|
2019 — n = 1336 |
2020 — n = 1409* |
|
|
Note: SD = standard deviation. |
||
| Gender | ||
| Male | 768 (57.5) | 776 (55.7) |
| Female | 568 (42.5) | 626 (44.4) |
| Age (years) | ||
| 0–5 | 600 (45.0) | 659 (46.8) |
| 6–9 | 489 (36.6) | 493 (35.0) |
| ≥ 10 | 247 (18.5) | 253 (18.0) |
| Mean ± SD | 6.39 ± 3.70 | 6.41 ± 3.77 |
| Presence of pain | ||
| Yes | 793 (59.4) | 987 (70.0)* |
| No | 543 (40.6) | 415 (29.5) |
| Presence of infection | ||
| Yes | 239 (17.9) | 357 (25.3)* |
| No | 1097 (82.1) | 1052 (74.7) |
| COVID symptoms | ||
| Yes | 27 (1.9) | |
| No | 1230 (87.3) | |
| Unknown | 152 (10.8) | |
During the first wave of the pandemic, the number of dental emergency visits remained stable until April 2020, then increased in May 2020 (Figure 1). The latter period is considered the peak of the pandemic in Canada, with an increase of 62.2% in emergency visits compared with the pre-pandemic period (p < 0.01). A gradual decrease in pediatric dental emergency visits started in late June 2020, but numbers remained similar to those of the pre-pandemic period.
Figure 2 shows changes in the diagnoses associated with the emergency dental visits. The number of caries-related visits significantly increased in the pandemic period (124% increase; p = 0.01) compared with the pre-pandemic period (Figure 2A). The number of dental trauma-related visits did not change (Figure 2B). A slight decrease was observed in the number of emergency visits for non-urgent problems early in the pandemic period (33% in April and 34% in May 2020). Non-urgent problems were defined as dental conditions that did not require immediate intervention (i.e., soft tissue pathologies, eruption disturbances, failed minor restorations and orthodontic appliances). However, the proportion of emergency visits associated with non-urgent problems during the first year of the pandemic did not differ from the pre-pandemic period.
In terms of management of pediatric dental emergencies, a significant increase occurred in the number of visits that were deferred during the pandemic period (“No treatment”; p < 0.01; Figure 3). Despite an increase in the number of dental extractions early in the pandemic period (52.5%; p = 0.02), the number of visits resulting in extractions was similar between pre-pandemic and pandemic periods. A slight reduction in the number of pulp therapy treatments was also observed during the early pandemic; however, this result was not significant.
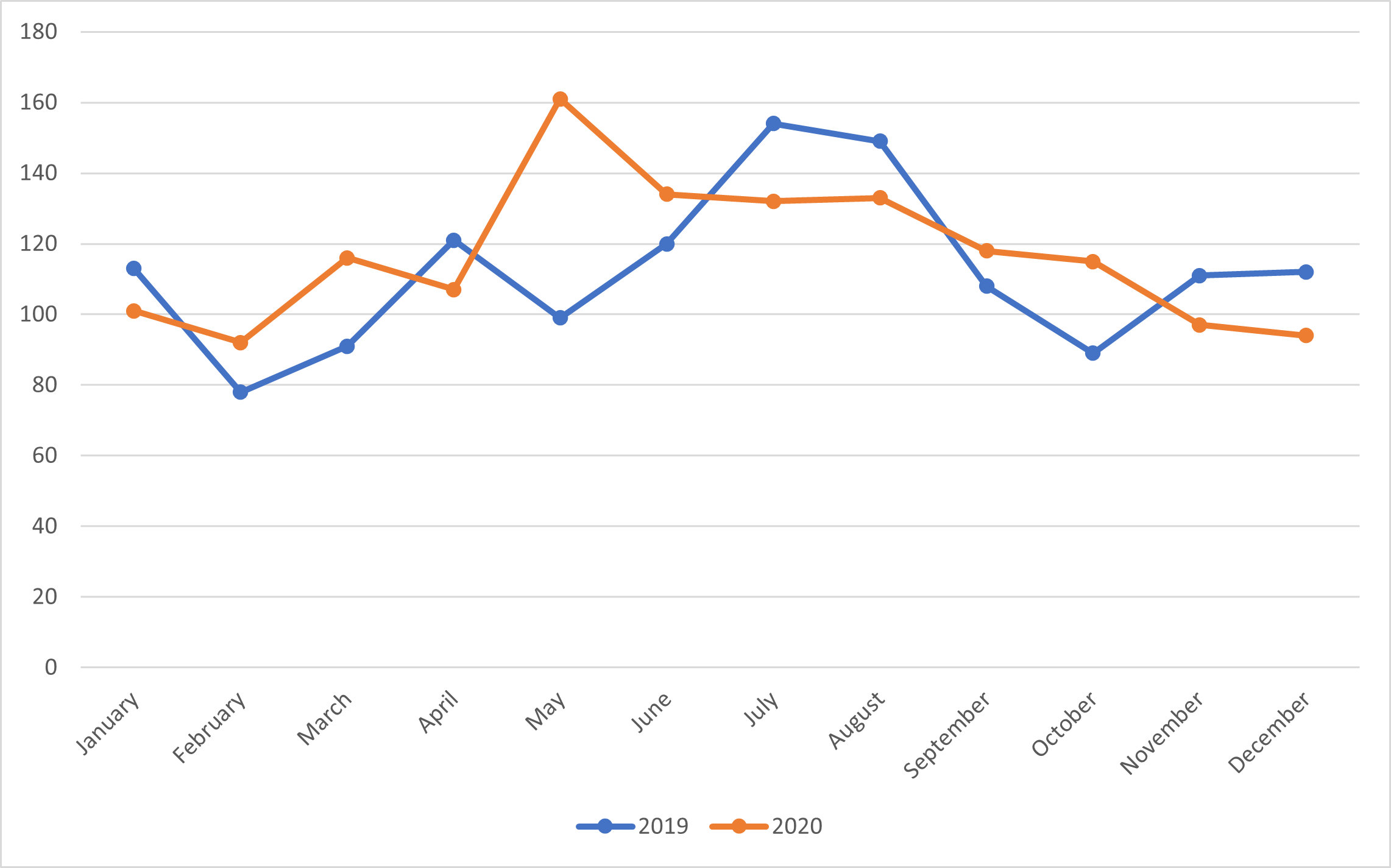
Figure 1: Number of pediatric dental emergency visits per month before (2019) and during (2020) the COVID-19 pandemic.
Figure 2: Number of dental emergency visits represented by children presenting for (A) caries-related problems; (B) traumatic dental injuries; and (C) non-urgent problems before (2019) and during (2020) the COVID-19 pandemic.
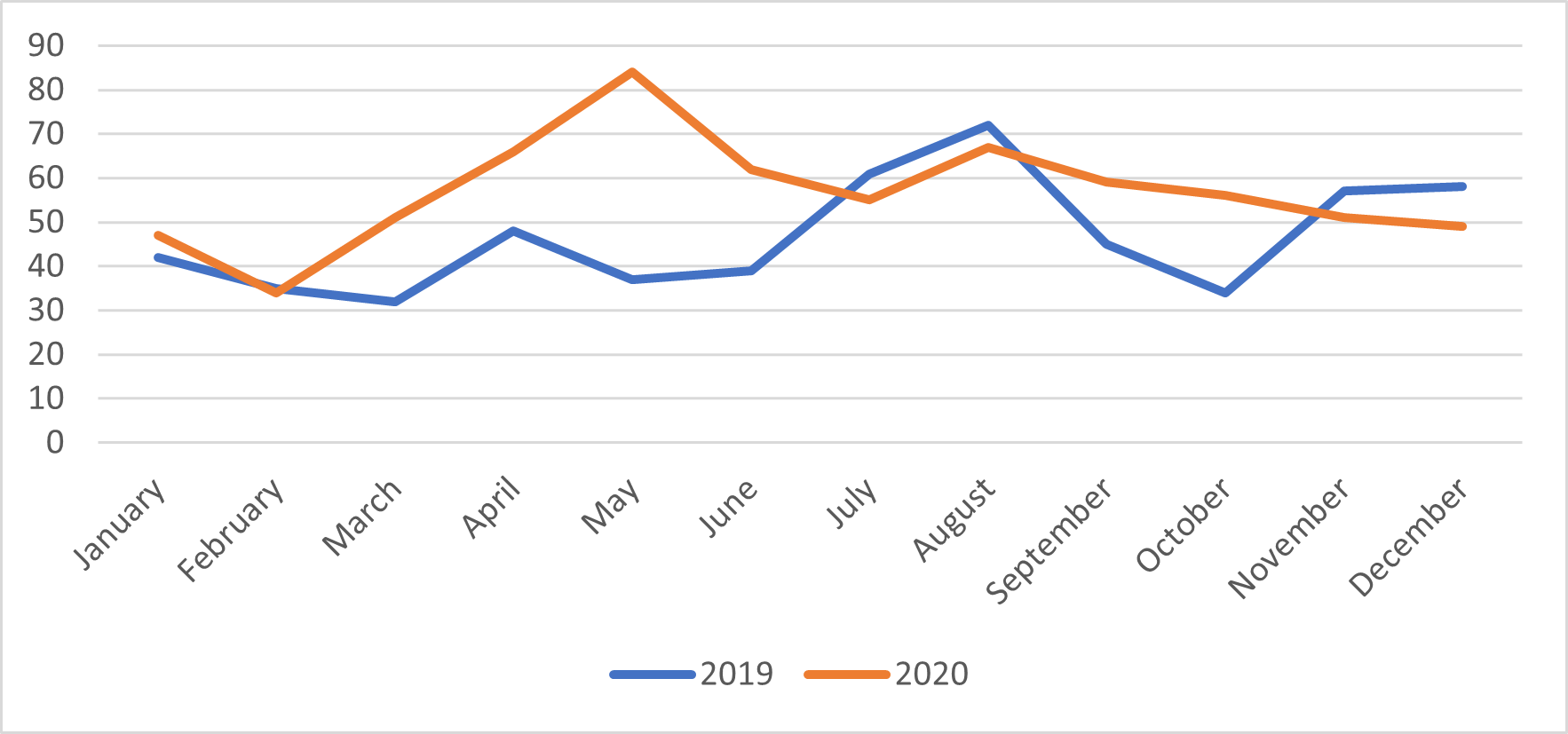
Figure 2A
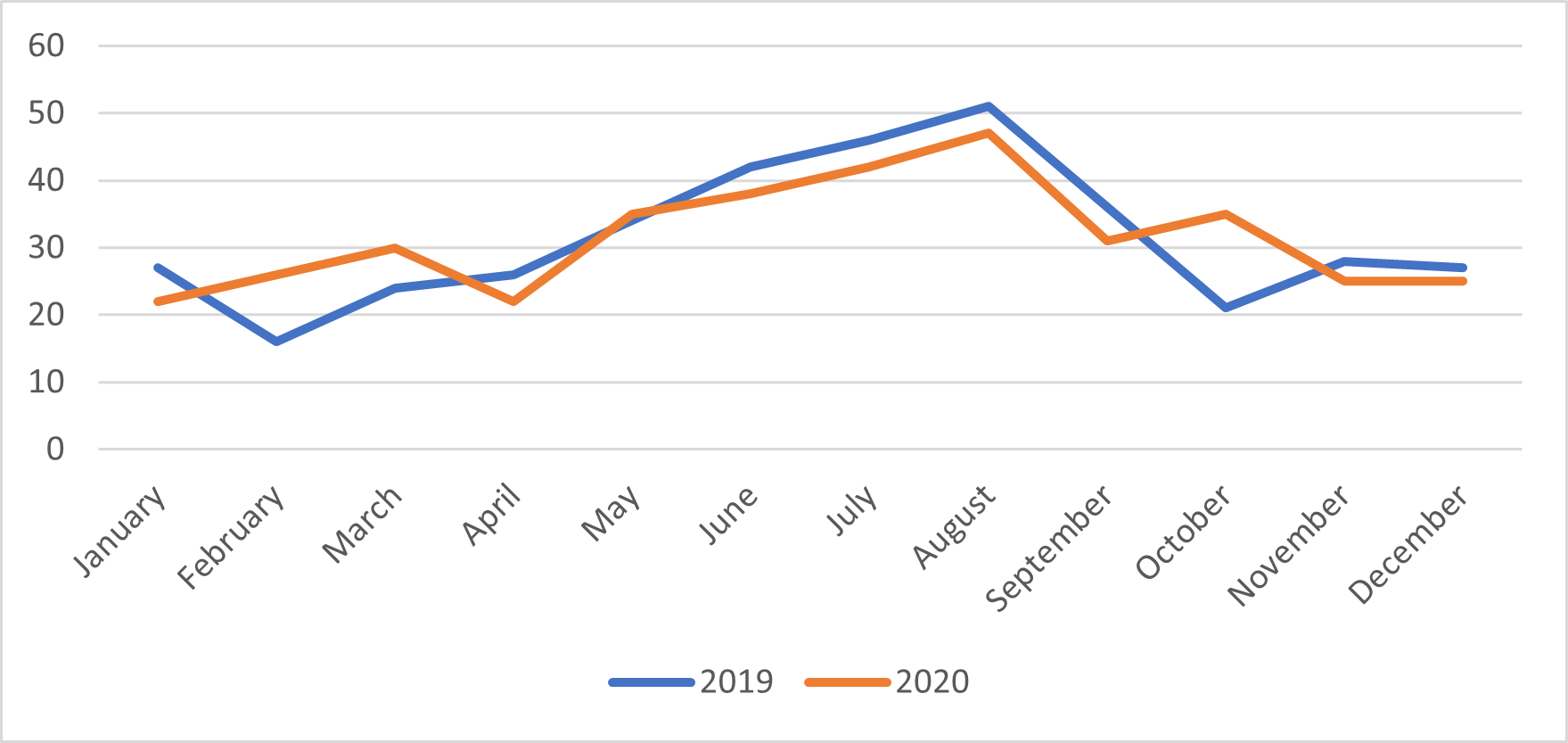
Figure 2B
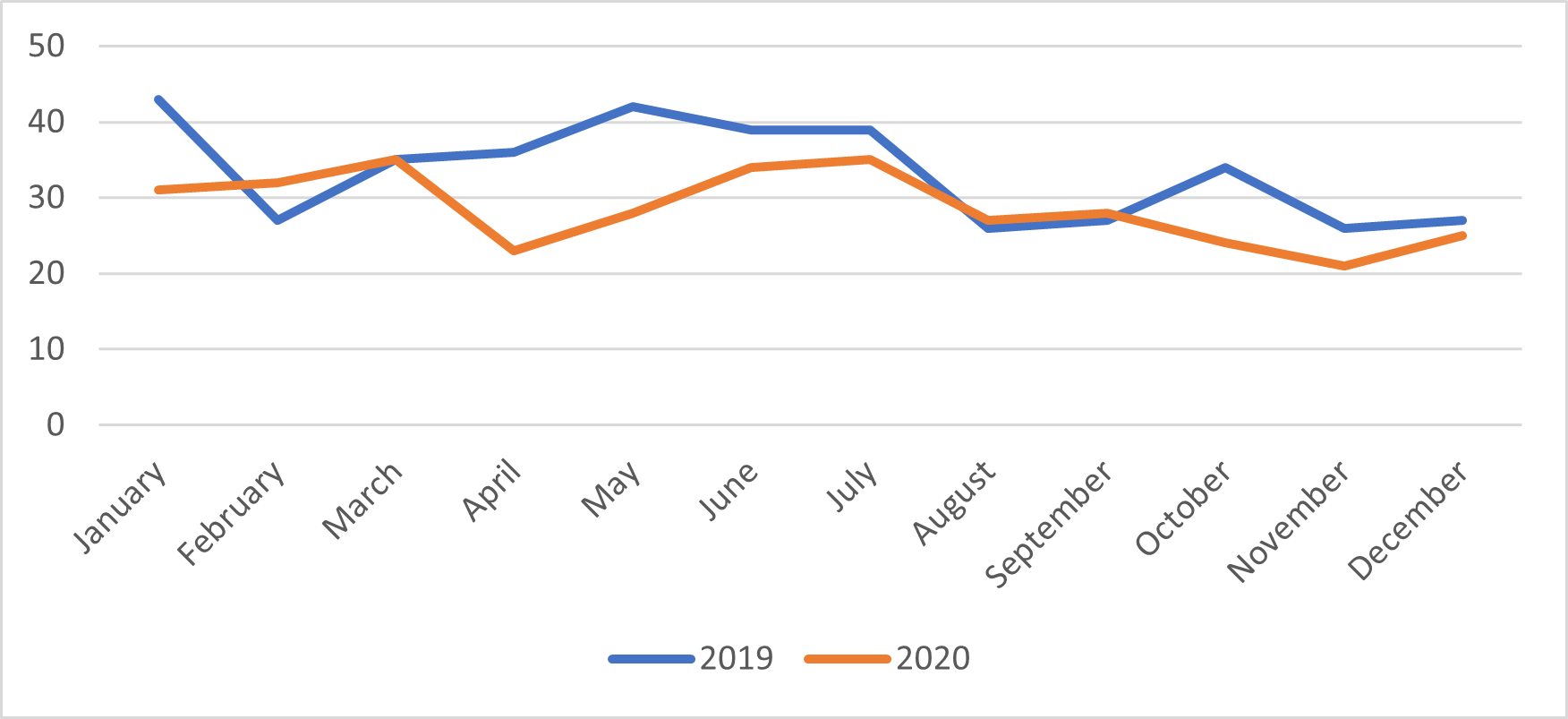
Figure 2C
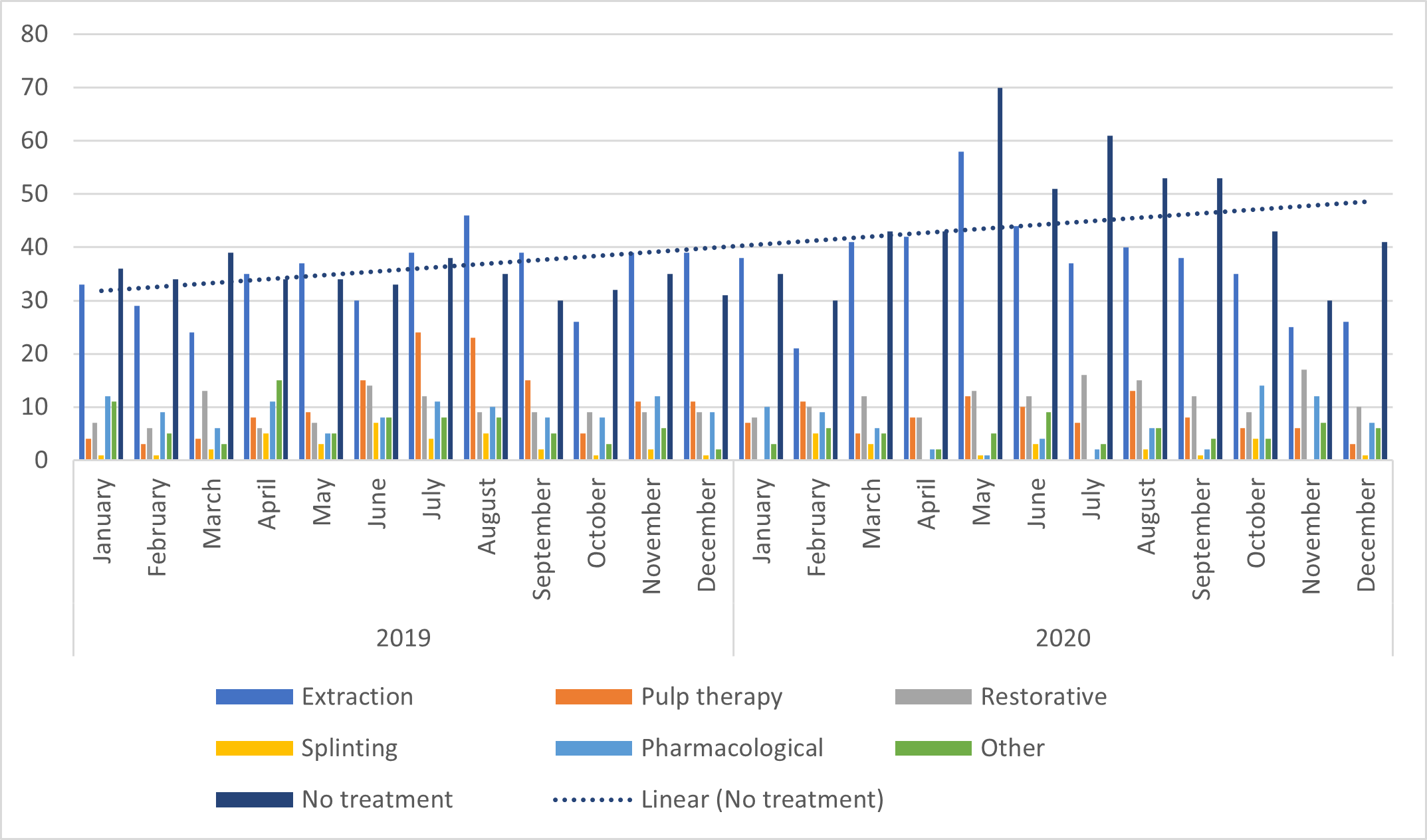
Figure 3: Management of pediatric dental emergencies before (2019) and during (2020) the COVID-19 pandemic.
Note: The dotted line is the linear trendline. It shows that "no treatment" increased during the study period.
Discussion
The results of this study indicate that the number of pediatric dental emergencies during the first wave of COVID-19 increased by 21% compared with the pre-pandemic period. A significant surge of 62.2% was noted for May 2020, the peak of the pandemic first wave in Canada. Similarly, a study from a tertiary care centre for dental medicine in Switzerland found an 8% increase in daily volume of dental emergencies among adult patients.11 Conversely, a reduction in the number of dental emergency visits during the lockdown period has been reported in India,13 Italy,8 Turkey14 and China.9 These reductions are commonly explained by implementation of government-imposed restrictions after declaration of the pandemic that severely limited access to dental care, as well as population fear of COVID-19 exposure. Furthermore, the widespread use of teledentistry and remote pharmaceutical prescriptions to avoid burdening emergency medical departments may also have played a role in reduction of visits.
The state of emergency declared by the Quebec government on March 14, 2020, led to the deferral of all non-urgent dental care to a later date4 and the closing of all dental offices in the province. This may explain the increased number of pediatric dental emergencies found in this study, as the MCH was one of the only pediatric tertiary care centres allowed to provide emergency dental care in Montreal during the first wave of the pandemic.
The acuity of dental conditions seen at the MCH also increased during the first wave. Delays in treatment caused by initial restrictions may have contributed to the worsening of dental conditions (i.e., dental abscess). The significant increase in the number of dental extractions observed in this study during the first wave could be explained by the possible worsening of patients’ condition and because an extraction is a non-aerosol-generating procedure. This same trend was also noted in 2 other studies from Switzerland, the United Kingdom and Italy,8,11 where they observed more extractions during both the lockdown and post-lockdown periods. Dental extraction was also the most common treatment for adult patients in a recent study from British Columbia.12
In addition, we found a significant increase in the number of pediatric dental emergency visits not receiving immediate treatment (“no treatment”) during the first wave of the pandemic. This delay might explain the increase in the number of dental extractions found in our study during the pandemic period.
Of interest, rates of visits for pediatric traumatic dental injuries (TDIs) were similar in both pre-pandemic and pandemic periods. Our results differ from previous studies that found a significant decrease in emergency TDI cases during the lockdown period, then a significant increase after the end of lockdown.7,10,12,15 The authors explained their findings as a possible increase in physical activities and leisure sports after the lockdown.8,11,13 Given the changes in societal and family dynamics imposed after the declaration of the pandemic,16 including work-from-home policies and closure of daycares/schools, parents had difficulty supervising their children. Therefore, we postulate that the similar trends in TDI in the pre-pandemic and pandemic periods noted in our study may be a result of accidents in the home environment. In addition, the declaration of the COVID-19 pandemic in Canada occurred in spring, when there is still snow and ice on the ground in Montreal, and, thus, less outdoor activity than in summer. A previous study at our hospital showed a higher incidence of dental trauma in the summer months.17
Despite Quebec’s publicly funded program providing limited oral health coverage for children less than 10 years, a recent study at our institution showed that the use of the pediatric emergency department for caries-related dental problems has increased in the last decade.17 This shows that Quebec families may still be seeking dental care for their children only in response to pain or swelling. This may be a result of barriers related to access to care, lack of a dental home or low oral health literacy.
During the first wave of the pandemic, the ability of our dental division to provide adequate care was hindered. To limit the spread of the pandemic, Canadian government bodies required the use of enhanced personal protective equipment (PPE) and negative pressure chambers for all aerosol-generating procedures. The division had limited access to PPE because of widespread concern over shortages. In addition, strict guidelines as to what was considered a dental emergency were provided by the Order of Quebec Dentists (ODQ).5 It is worth mentioning that teledentistry was adopted by the division as a way to triage patients and better manage dental emergencies, especially during the first wave of the pandemic.
Limitations
This study has potential limitations. First, data were collected from a single tertiary care pediatric hospital in Quebec and, therefore, the results cannot be generalized. However, this centre was one of the only pediatric hospitals designated to see dental emergencies in Montreal. Second, because of the retrospective nature of this study, data were limited to information found in charts. Third, patients seen by hospital physicians and discharged home without referral or consultation by the division of dentistry were not included. Finally, data on the use of teledentistry during the first wave of the pandemic were not captured in our study; thus, future studies are needed to assess the impact of teledentistry in the management of dental emergencies during the COVID-19 pandemic.
Despite these limitations, to our knowledge, this study is the first to describe the pattern of pediatric dental emergencies at a major pediatric hospital in Quebec during the COVID-19 pandemic. Our findings add to the current literature assessing rates of pediatric dental emergencies during the first year of the COVID-19 pandemic.
Conclusions
The overwhelming impact of the COVID-19 pandemic is ongoing and its onset caused a disruption in the provision of pediatric dental care. Our study shows that there was a significant increase in the rate of dental emergencies during the first wave of the pandemic. The increase was mainly a result of patients seeking emergency care for dental infections, where limited care was available in the community setting.
Based on these findings, access to dental emergencies was affected for patients seeking care for the period corresponding to the first wave of the pandemic. The COVID-19 pandemic is an ongoing global public health crisis, and it remains to be seen how the provision of pediatric dental care might be further affected in the future. However, increased public health measures that ensure a safe environment for staff and patients and adaptation to the pandemic are important in ensuring continued quality of care for patients.
THE AUTHORS
 |
Dr. Bacho is pediatric dentist fellow, division of dentistry, department of pediatric surgery, Montreal Children’s Hospital, Montreal, Canada. |
 |
Dr. Mounir is dental staff, division of dentistry, department of pediatric surgery, Montreal Children’s Hospital, Montreal, Canada. |
 |
Dr. Chan is general practice residency director, division of dentistry, department of pediatric surgery, Montreal Children’s Hospital, Montreal, Canada. |
 |
Dr. Ferraz dos Santos is research director, division of dentistry, department of pediatric surgery, Montreal Children’s Hospital; and assistant professor, faculty of dental medicine and oral health sciences, McGill University, Montreal, Canada. |
Corresponding author: Dr. Beatriz Ferraz dos Santos, Division of Dentistry, Department of Pediatric Surgery, Montreal Children’s Hospital, 1040 Atwater Avenue, Montreal, QC H3Z 1X3. Email: beatriz.ferrazdossantos@mcgill.ca
Acknowledgements: We thank all the staff in the Division of Dentistry, Montreal Children’s Hospital, for all their efforts during the COVID-19 pandemic.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- COVID-19 — China. Geneva: World Health Organization; 2020 . Available: www.who.int/emergencies/disease-outbreak-news/item/2020-DON233 (accessed 2023 Aug. 6).
- Pandémie de la COVID-19 — Le Québec sur pause pour trois semaines. Québec: Gouvernement du Québec; 2020. Available: www.quebec.ca/nouvelles/actualites/details/pandemie-de-la-covid-19-le-quebec-sur-pause-pour-trois-semaines (accessed 2023 Aug. 6).
- Coronavirus disease (COVID-19): outbreak update. Ottawa: Government of Canada; 2020. Previously available: canada.ca/en/public-health/services/coronavirus-disease-covid-19 (accessed 2021 Mar 9, URL no longer active).
- Managing the COVID-19 health crisis. Montréal: Ordre des dentistes du Québec; 2020. Previously available: odq.qc.ca/Portals/DossierSante/covid-19 (accessed 2021 Jan 12, URL no longer active).
- Decision tree. Montréal: Ordre des dentistes du Québec; 2020. Previously available: odq.qc.ca/Portals/DossierSante/Arbre-Decisionnel-Modifications (accessed 2020 May 8, URL no longer active).
- ADA recommending dentists postpone elective procedures. Chicago: American Dental Association; 2020. Available: www.ada.org/en/publication/adanews/interim-guidance (accessed 2021 Jan 12).
- Meng L, Hua F, Bian Z. Coronavirus disease 2019 (COVID-19): emerging and future challenges for dental and oral medicine. J Dent Res. 2020;99(5):481-7.
- Cagetti MG, Balian A, Camoni N, Campus G. Influence of the COVID-19 pandemic on dental emergency admissions in an urgent dental care service in north Italy. Int J Environ Res Public Health. 2021;18(4):1812.
- Guo H, Zhou Y, Liu X, Tan J. The impact of the COVID-19 epidemic on the utilization of emergency dental services. J Dent Sci. 2020;15(4):564-7.
- Samuel SR, Mathew MG, Suresh SG, Varma SR, Elsubeihi ES, Arshad F, et al. Pediatric dental emergency management and parental treatment preferences during COVID-19 pandemic as compared to 2019. Saudi J Biol Sci. 2021;28(4):2591-7.
- Eggmann F, Haschemi AA, Doukoudis D, Filippi A, Verna C, Walter C, et al. Impact of the COVID-19 pandemic on urgent dental care delivery in a Swiss university center for dental medicine. Clin Oral Investig. 2021;25(10):5711-21.
- Tong NR, Park J, Carlisle S, Poh CF. Characteristics of emergent and essential dental services in university and hospital-based settings during COVID-19 pandemic in Vancouver, Canada. J Can Dent Assoc. 2021;87:l13.
- Kumar U, Gupta A, Goyal A, Gauba K. Impact of covid-19 pandemic on characteristics of dental emergencies and treatment services at tertiary care centre. Saudi Dent J. 2021;33(8):1018-23.
- Ustun N, Akgöl BB, Bayram M. Influence of COVID-19 pandemic on paediatric dental attendance. Clin Oral Investig. 2021;25(11):6185-91.
- Yang YT, Zhang W, Xie L, Li ZB, Li Z. Characteristic changes of traumatic dental injuries in a teaching hospital of Wuhan under transmission control measures during the COVID-19 epidemic. Dent Traumatol. 2020;36(6):584-9.
- Wong CKH, Wong JYH, Tang EHM, Au CH, Lau KTK, Wai AKC. Impact of national containment measures on decelerating the increase in daily new cases of COVID-19 in 54 countries and 4 epicenters of the pandemic: comparative observational study. J Med Internet Res. 2020;22(7):e19904.
- Ferraz Dos Santos B, Dabbagh B. A 10-year retrospective study of paediatric emergency department visits for dental conditions in Montreal, Canada. Int J Paediatr Dent. 2020;30(6):741-8.