Abstract
Introduction: Establishing dental homes for children at an early age is an important step toward instilling good oral health practices and changing trajectories of oral health. The purpose of this study was to determine how accredited dental and dental hygiene programs in Canada prepare students in the areas of infant, toddler and prenatal oral health.
Methods: An electronic questionnaire was sent to associate deans (academic), program directors or curriculum directors of accredited dental (n = 10) and dental hygiene (n = 39) programs. Participants were asked about infant, toddler and prenatal oral health curricula taught at their institution. Descriptive statistics and bivariate analyses were used to assess the results. A p value ≤ 0.05 was considered significant.
Results: Representatives of 10 dental (100%) and 25 dental hygiene (64.1%) programs responded. All dental and 56% of dental hygiene programs recommend a first visit by 12 months. Infant and toddler oral health was noted as a component of most schools' curriculum. Barriers to teaching about or providing clinical experiences in infant and toddler oral health include lack of time, patients, program resources and finances. Most dental (70%) and dental hygiene (82.6%) programs include prenatal oral health as a component of their curriculum, yet only 40% of responding dental and 70% of dental hygiene programs reported having designated time in their curriculum for it. Barriers preventing programs from teaching or providing clinical experiences regarding prenatal oral health include lack of time and patients.
Conclusions: Many, but not all dental professional programs are teaching their students about the recommended age for a first dental visit. Better adherence to national guidelines will require programs to address current barriers impeding learning about this important topic and to provide creative opportunities for students regarding prenatal and infant and toddler oral health.
The concept of a dental visit by 12 months of age was first proposed by the American Academy of Pediatric Dentistry in 1986.1 Today, professional organizations recommend a first visit coinciding with the eruption of the first tooth or no later than 12 months of age.2-4 The rationale is based primarily on the argument that such a visit establishes a preventive and cost-effective practice for the caregiver and provides long-term benefits for the child.5
Although the Canadian Dental Association (CDA) first endorsed the visit at 12 months in 2001,1 many practitioners and parents remain uninformed.6,7 The CDA recently announced that improving access to first dental visits is a priority approach to address oral health disparities facing young children.
Early preventive visits, particularly for families at high risk, can help reduce the number of children developing caries and promote preventive care.8-10 However, one of the challenges regarding access to care is the limited number of dentists willing to see infants (≤ 12 months) and toddlers (1–3 years).6,11 A recent survey revealed that some general dentists are willing to see low-risk infants and toddlers, but not those with obvious dental disease.12 Parents who attempt to obtain an early consultation for their child may become discouraged, as some practitioners refuse to see any children under 3 years of age.13
Although many early childhood oral health care advocates suggest an interprofessional approach, we must first understand whether this concept and practice are being taught in undergraduate oral health curricula in Canada. Given the important link between a mother's oral health and that of her child, further understanding of what is taught about prenatal oral health is essential. Without an engaged dental workforce united on this topic, our medical colleagues will continue to become increasingly frustrated by the lack of dental homes for their pediatric patients.12-14
The Commission on Dental Accreditation of Canada (CDAC) establishes requirements for accreditation to ensure that graduates are capable of addressing the oral care needs of the Canadian public. A search of the CDAC accreditation requirements for a graduating dental student found none specifically addressing infant oral health. Section 2.3.12 of the accreditation requirements for Doctor of Dental Surgery or Doctor of Dental Medicine programs states, "Graduates must be competent in the management of the oral health care of the child, adolescent, adult and geriatric patient."15 The document does not identify management of infant oral health as a separate requirement, although its inclusion is implied. Similarly, there is no mention of specific requirements relating to infant oral health for a graduating dental hygiene student; these graduates must be "competent to manage health promotion and oral health care for a range of clients within the life cycle, including children, adolescents, adults, and seniors."16 Because dental development and progression of dental disease during childhood vary greatly from birth to adolescence, the lack of specific inclusion of the infant and toddler age groups may lead to their omission from curricula.
The purpose of this study was to determine the extent to which accredited dental and dental hygiene programs in Canada prepare future clinicians in the areas of infant, toddler and prenatal oral health.
Methods
The study population included an associate dean (academic), program director, chair of pediatric dentistry or curriculum director of the 10 accredited dentistry and 39 dental hygiene programs in Canada. Names of all eligible accredited programs were obtained from the CDAC.17 The University of Manitoba's Health Research Ethics Board approved this study.
In June 2012, a questionnaire was sent via Survey Monkey to our identified contact at each institution (n = 49). Completing the online questionnaire constituted informed consent. For French-speaking educators, a professionally translated French version of the questionnaire was sent. Reminders along with a questionnaire link were sent to all non-responders monthly; the final reminder was sent in February 2013.
The questionnaire was developed by the project team to collect information on whether, and to what extent, programs were educating students in infant, toddler and prenatal oral health. Specifics explored methods used, hours dedicated to each method and materials used to educate students.
Information was exported to an Excel (Microsoft Corp., Redmond, Wash., USA) spreadsheet and analyzed using NCSS v. 8 (NCSS LLC, Kaysville, Utah, USA). Descriptive statistics (frequencies, means and standard deviations [SD]) and t-tests were conducted with Bonferroni correction as required. A p value ≤ 0.05 was considered significant.
Results
Description of Participants
Representatives of 10 dental (100%) and 25 dental hygiene programs (64.1%) responded. Most (69.6%) of the dental hygiene programs were college based, while the remainder were university based (17.4%) or private (13.0%).
Infant and Toddler Oral Health Curriculum
According to respondents, all 10 dental schools recommend that a child's first dental visit take place by 12 months of age. However, only 56% of dental hygiene programs recommend visits by this milestone. Most respondents (90% dentistry, 84% dental hygiene) indicated that infant and toddler oral health is an explicit component of their school's curriculum (Table 1). All respondents indicated that time is designated in their curriculum for this topic. Time devoted to didactic instruction varies; dentistry programs: 6.9 ± 5.7 h (mean ± SD), range 2–20 h; dental hygiene programs: 5.5 ± 2.8 h, range 1–10 h, but the difference between these programs is not significant (p = 0.46).
| Question | Dentistry, no. (%) |
Dental hygiene, no. (%) |
|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | ||
| In your school's curriculum, what age is recommended for a child's first dental visit? | ||
| 6 months | 0 (0) | 5 (20) |
| By 12 months of age or the 1st birthday | 10 (100) | 9 (36) |
| By 24 months of age or the 2nd birthday | 0 (0) | 6 (24) |
| By 36 months of age or the 3rd birthday | 0 (0) | 2 (8) |
| > 36 months of age or after the 3rd birthday | 0 (0) | 3 (12) |
| Are infant and toddler oral health explicitly noted as a component of your school's curriculum? | ||
| Yes | 9 (90) | 21 (84) |
| No | 1 (10) | 4 (16) |
| Are infant and toddler oral health explicitly noted as a component of your school's core competencies? | ||
| Yes | 4 (40) | 14 (56) |
| No | 6 (60) | 11 (44) |
| Do you have designated time in your school's curriculum for teaching infant and toddler oral health? | ||
| Yes | 10 (100) | 25 (100) |
| No | 0 (0) | 0 (0) |
| Does your school offer additional elective training in infant and toddler oral health education? | ||
| Yes | 4 (40) | 1 (4.4) |
| No | 6 (60) | 22 (95.6) |
| Amount of time devoted to infant and toddler oral health in your school's total didactic curriculum, h (mean ± standard deviation) | 6.9 ± 5.7 | 5.5 ± 2.8 |
Few programs offer additional elective training. Only 1 dental hygiene (4.4%) and 4 dentistry schools (40%) reported offering such opportunities. Such training most commonly takes place in community programs, public health clinics and pediatric dentistry clinics, with considerable variation in hours of exposure (11.8 ± 12.3 h, range 3–30 h).
In terms of the time devoted to various teaching methods, lectures and seminars were the most common didactic approaches followed by clinical care and clinical observation only (Table 2). There were no apparent differences between dental and dental hygiene programs in amount of teaching time. Although dental hygiene respondents reported more hours devoted to didactic instruction, Bonferroni correction revealed that the difference was not significant.
| Teaching method | Dentistry, h (mean ± SD; range) |
Dental hygiene, h (mean ± SD; range) | p* |
|---|---|---|---|
| *Bonferroni correction to address inflated type I error. Significance then set at p ≤ 0.008; hence, no comparisons are statistically significant. | |||
| Lectures and seminars | 3.0 ± 0.67 (2–4) |
4.6 ± 2.6 (1–12) |
0.01 |
| Video, Internet or web-based learning | 0.4 ± 0.97 (0–3) |
0.7 ± 0.97 (0–3) |
0.43 |
| Clinical (observation only) | 2.2 ± 3.1 (0–10) |
1.3 ± 3.1 (0–10) |
0.45 |
| Clinical dental screening | 0.7 ± 1.1 (0–3) |
1.7 ± 3.3 (0–12) |
0.19 |
| Clinical patient care (prevention and/or restorative) | 2.5 ± 2.8 (0–9) |
3.5 ± 4.4 (0–12) |
0.52 |
| Other teaching methods | 0.3 ± 0.9 (0–3) |
0.7 ± 2.2 (0–10) |
0.48 |
Less than a third of dental and dental hygiene programs reported that all students receive clinical hands-on experience in performing infant and toddler examinations (Table 3). Most responding dental (60.0%) and dental hygiene programs (52.2%) rely on their institution's clinic to provide these opportunities, while others send students to primary care clinics, daycares and public health settings. Of those who provide hands-on examination experiences to some or all of their students, most dental programs (5/9) reported that fewer than 50% of their students receive 1 or more clinical hands-on experiences while most dental hygiene programs (8/14) reported that ≥ 75% of their students have such opportunities (Table 3).
| Question | Dentistry, no. (%) |
Dental hygiene, no. (%) |
|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | ||
| Clinical experience | ||
| Clinical hands-on experience: infant/toddler oral health examinations | ||
| All students have experience | 3 (30) | 7 (30.4) |
| Variable experience for students | 6 (60) | 7 (30.4) |
| No experience for students | 1 (10) | 9 (39.1) |
| One or more infant/toddler clinical hands-on experiences | ||
| < 5% | 0 (0.0) | 2 (14.3) |
| 5–10% | 3 (33) | 1 (7.1) |
| 25–49% | 2 (22) | 0 (0.0) |
| 50–74% | 1 (11) | 3 (21.4) |
| 75–100% | 3 (33) | 8 (57.1) |
| Collaboration to expose students to infants/toddlers (all that apply) | ||
| Primary care clinics | 3 (30) | 5 (20) |
| Community dental clinics | 5 (50) | 4 (16) |
| Public health settings or programs | 2 (20) | 15 (60) |
| Pediatric dentists (private practice) | 1 (10) | 3 (12) |
| Daycares | 1 (10) | 14 (56) |
| Other (please specify): | 3 (30) | 2 (8) |
| Didactic experience | ||
| Amount of toothpaste | ||
| Yes | 10 (100) | 23 (100) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 0 (0) |
| Benefits and frequency of fluoride varnish to prevent and arrest caries | ||
| Yes | 10 (100) | 20 (87.0) |
| No | 0 (0) | 1 (4.4) |
| Unsure | 0 (0) | 2 (8.7) |
| Apply fluoride varnish | ||
| Yes | 9 (90) | 18 (78.3) |
| No | 0 (0) | 4 (17.4) |
| Unsure | 1 (10) | 1 (4.4) |
| Discuss proper diet with caregivers? | ||
| Yes | 9 (90) | 19 (82.6) |
| No | 1 (10) | 2 (8.7) |
| Unsure | 0 (0) | 2 (8.7) |
| Perform and position for an oral health examination | ||
| Yes | 10 (100) | 18 (78.3) |
| No | 0 (0) | 2 (8.7) |
| Unsure | 0 (0) | 3 (13.0) |
| Recognize dental caries | ||
| Yes | 10 (100) | 22 (95.7) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 1 (4.4) |
| Curriculum content (professional policies and guidelines included in the infant/toddler curriculum) | ||
| Dental home | ||
| Yes | 10 (100) | 11 (47.8) |
| No | 0 (0) | 5 (21.7) |
| Unsure | 0 (0) | 7 (30.4) |
| Infant oral health care | ||
| Yes | 10 (100) | 19 (82.6) |
| No | 0 (0) | 3 (13.0) |
| Unsure | 0 (0) | 1 (4.4) |
| Definition of early childhood caries | ||
| Yes | 10 (100) | 21 (91.3) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 2 (8.7) |
| Caries-risk assessment tools | ||
| Yes | 9 (90) | 22 (95.6) |
| No | 1 (10) | 0 (0) |
| Unsure | 0 (0) | 1 (4.4) |
Many respondents indicated that their programs expose students to working with high-risk infant and toddler populations, e.g., Aboriginal (dentistry 40%, dental hygiene 32%), low-income (80%, 72%), refugees (60%, 20%). Dentistry and dental hygiene programs appear to have limited inter-professional learning opportunities for their students (30%, 47.8%).
Barriers to teaching about or providing clinical experiences in infant and toddler oral health include lack of time, patients, program resources and finances (Fig. 1).
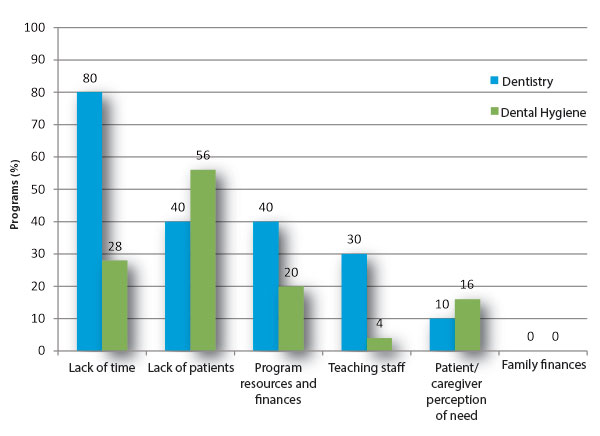 Figure 1: Barriers to teaching or providing clinical experience in infant and toddler oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Figure 1: Barriers to teaching or providing clinical experience in infant and toddler oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Key policies and clinical guidelines related to infant and toddler oral health appear to be present in curricula (Table 3). Other concepts related to infant oral health, such as the use of fluoride toothpastes and varnishes, infant feeding practices and caries diagnosis, are also taught (Table 3). Most programs recommend fluoridated toothpaste for infants and toddlers (dentistry 80%, dental hygiene 65.2%). Nearly all respondents were aware that their program discusses professional recommendations for a first dental visit (dentistry 100%, dental hygiene 91.3%) and were aware of the CDA's position statement on early childhood caries2 (dentistry 100%, dental hygiene 82.6%). All respondents reported being aware of the CDA's position statement on fluoride18 (dentistry 100%, dental hygiene 100%).
All respondents indicated that their curriculum teaches students about the relationship between bottle feeding and oral health, while 90% of dental and 87% of hygiene programs reported teaching students about breastfeeding and oral health.
Prenatal Oral Health Curriculum
Respondents noted that in most dental (70%) and dental hygiene (82.6%) programs, prenatal oral health is a component of the curriculum (Table 4). Time is designated in the curriculum of 40% of dental and 69.6% of hygiene programs for teaching prenatal oral health. Educating students about the relation between periodontal disease during pregnancy and premature birth and low birthweight was commonly reported (dentistry 70%, dental hygiene 95.7%). Most respondents also reported that their program informs students about the role of prenatal nutrition in infant oral health (dentistry 80%, dental hygiene 91.3%). All reported teaching about bacterial transmission from mother to infant.
Details on methods used and time devoted to prenatal oral health appear in Table 5. Barriers to teaching or providing clinical experiences in prenatal oral health include lack of patients and time in the curriculum (Fig. 2).
| Question | Dentistry, no. (%) | Dental hygiene, no. (%) |
|
|---|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | |||
| Explicitly noted as a component of your school's curriculum? | |||
| Yes | 7 (70) | 19 (82.6) | |
| No | 1 (10) | 3 (13.0) | |
| Unsure | 2 (20) | 1 (4.4) | |
| Explicitly noted as a component of your school's core competencies? | |||
| Yes | 4 (40) | 10 (43.5) | |
| No | 4 (40) | 10 (43.5) | |
| Can be done as an elective | 0 (0) | 1 (4.4) | |
| Unsure | 2 (20) | 2 (8.7) | |
| Designated time in your school's curriculum (either through your department or other departments)? | |||
| Yes | 4 (40) | 16 (69.6) | |
| No | 2 (20) | 4 (17.4) | |
| Unsure | 4 (40) | 3 (13.0) | |
| Contemplating adding prenatal oral health o curriculum? | |||
| Yes, within the next 12-24 months | 3 (30) | 5 (21.7) | |
| No | 1 (10) | 7 (30.4) | |
| Unsure | 6 (60) | 11 (47.8) | |
| Additional elective training in prenatal oral health education? | |||
| Yes | 0 (0) | 3 (13.0) | |
| No | 7 (70) | 20 (87.0) | |
| Unsure | 3 (30) | 0 (0) | |
| Students who have 1 or more prenatal clinical hands-on experiences, % | |||
| None | 5 (50) | 3 (13.0) | |
| < 5 | 0 (0) | 5 (21.7) | |
| 5–10 | 2 (20) | 3 (13.0) | |
| 11–24 | 0 (0) | 3 (13.0) | |
| 25–49 | 0 (0) | 2 (8.7) | |
| 50–74 | 0 (0) | 2 (8.7) | |
| 75–100 | 0 (0) | 4 (17.4) | |
| Unsure | 3 (30) | 1 (4.4) | |
| Which department(s) or discipline(s)/course(s) is/are responsible for teaching prenatal oral health? (check all that apply) | |||
| Periodontal | 2 (20) | 5 (20) | |
| General dentistry/operative dentistry | 0 (0) | 1 (4) | |
| Public health/community dentistry | 5 (50) | 17 (68) | |
| Pediatric dentistry | 7 (70) | 7 (28) | |
| Unsure | 2 (20) | 3 (12) | |
| Other (please specify): | 0 (0) | 9 (36) | |
| Amount of time in your school's total curriculum devoted to prenatal oral health, h (mean ± SD) | 2.6 ± 3.8 | 3.5 ± 2.5 | |
| Dentistry, h (mean ± SD; range) | Dental hygiene, h (mean ± SD; range) |
p value | |
|---|---|---|---|
| Lectures and seminars | 2.0 ± 3.1 (0–10) |
2.8 ± 2.3 (0–10) |
0.44 |
| Video, Internet or web-based learning | 0.0 ± 0.0 | 0.4 ± 0.9 (0–4) |
— |
| Clinical (observation only) | 0.0 ± 0.0 | 0.8 ± 2.4 (0–10) |
— |
| Clinical dental screening | 0.0 ± 0.0 | 0.8 ± 2.4 (0–10) |
— |
| Clinical patient care (prevention and/or restorative) | 0.0 ± 0.0 | 1.3 ± 2.5 (0–10) |
— |
| Other teaching methods | 0.0 ± 0.0 | 0.7 ± 2.2 (0–10) |
— |
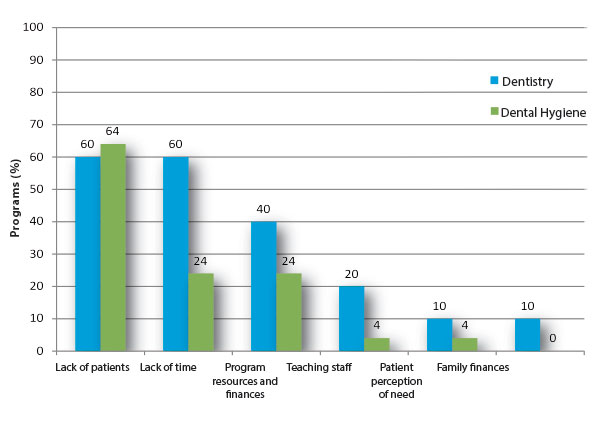 Figure 2: Barriers to teaching or providing clinical experience in prenatal oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Figure 2: Barriers to teaching or providing clinical experience in prenatal oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Discussion
This study is the first to examine Canada's dental curricula related to prenatal and early childhood oral health. Our study found that while efforts are made to teach students about these important topics in both didactic and clinical domains, variability in curricula exists, highlighting deficiencies in dental education in terms of adequately preparing the future dental workforce to care for young children. Unfortunately, few Canadian children benefit from early first visits,19 stressing the inconsistencies between clinical practice, current national guidelines and educational curricula.20
The question remains: how best can we assist dental educators to prepare dental professionals to care for pregnant women and very young children? Based on our findings, we propose that dental curricula consider didactic, clinical domain and system-wide changes, although inconsistencies also exist between clinical guidelines and practice.
Didactic Teaching
The amount of didactic teaching in prenatal and infant oral health reported by dentistry (70% and 100%, respectively) and dental hygiene (82.6% and 100%, respectively) programs is encouraging. Although responding dental hygiene programs reported more time in their curriculum for didactic teaching in infant and toddler oral health than dental schools, 44% of dental hygiene programs do not recommend a first visit by 12 months of age. These findings suggest the need for re-acquaintance with current clinical practice guidelines. A survey of Manitoba dentists found that only 58% were aware of the recommendation for a first dental visit.6 Although this proportion appears to have increased following a health promotion campaign by the profession (i.e., the Free First Visit program),7,21 such knowledge is key as it is a factor in increasing the odds of dentists accepting referrals in early childhood.22 Anecdotally, it was reported by co-authors FH and RH that a First Dental Visit campaign by the BC Dental Association that included hands-on workshops and development of online material, including an online learning tool for general dentists, has also led to increased numbers of dentists welcoming infants and toddlers to their offices.
With limited human resources for dental education,23,24 as verified in our survey, innovative ways to disseminate knowledge about current guidelines on prenatal and infant oral health could be helpful. Time could be better devoted to promoting clinical experiences in this area, a barrier noted by educators in our study. Development of standardized curricula using innovative web-based teaching methods, similar to that developed by the BC Dental Association, may provide students with a foundational level of knowledge.25 Evidence suggests that web-based delivery can produce learning outcomes equal to face-to-face education.26
Clinical Experience
Our study found that, although many programs teach about the timing of a first visit, less than a third offer hands-on experiences in performing assessments. This lack of clinical experience increases the possibility that students will not engage in these activities following graduation.24,27 Unfortunately, most of the hands-on clinical experience that students receive is with children 4 years of age and over.24,27
A recent Cochrane review of continuing medical education found that combining interactive and didactic formats is a more effective approach than either alone.28 This finding encourages the enhancement of undergraduate curricula to include hands-on training. Specific to dental education in early childhood, evidence suggests that comfort is a significant predictor of general dentists' stage of readiness to deliver preventive oral health services to this cohort. As practitioners' comfort increases, they were found to be 3.4 and 5.8 times more likely to perform these services than those contemplating and those unwilling to perform these services, respectively.29 Strategies to promote comfort and self-efficacy through clinical experiences during dental education have been shown to improve knowledge and confidence in performing these services for young children.30 In other areas of health care education, multiple exposures to procedures have been linked with increased student confidence.31
To provide these clinical experiences, suitable patients are needed. Lack of patients was mentioned by educators in our study as 1 of the top 2 barriers to teaching and providing clinical experience in prenatal and infant and toddler oral health. This barrier has previously been reported, and promoting creative collaborations outside dental settings should be explored.24 Interprofessional educational opportunities in primary care settings with pediatrics, obstetrics and family medicine components may expose students to these populations. Not only could these opportunities enhance training, but they may also foster awareness of oral health among non-dental professionals and lead to better coordination of care and establishing and maintaining dental homes.
Systems-Based Issues
To ensure that comprehensive education in prenatal and early childhood oral health is part of dental programs, the CDAC's current accreditation requirements should be reviewed and amended to include pregnant women, infants and toddlers and other vulnerable patient groups. This will help promote their adoption into the global and enabling objectives of dental curricula. Another useful approach may be to supplement each program's curriculum with an innovative online module on infant and toddler oral health. The current evolution of dental education beyond the traditional surgical to a more preventive approach and the increased emphasis on the medical rather than the surgical management of caries should lead to more universal adoption of early intervention. Consideration of developing mini pediatric dentistry rotation opportunities for senior students interested in general dentistry rather than a specialty-focused career may assist with workforce issues, as such "super" general dentists will provide the greatest safety net for pregnant women and children.24,30,32
National oral health campaigns targeting the public can help address the perception, as identified in our study, that parents lack awareness of the need for early dental care. This finding is consistent with pediatric dentists citing parents' diminished value on infant oral health as the main barrier for not caring for young children.33 A public campaign of the CDA and CDHA or provincial member services organizations promoting the first dental visit would help change perceptions and have an impact on all aspects of clinical practice. In 2009, the Journal of the Canadian Dental Association published a short article along with a complementary PowerPoint presentation to teach dentists how to perform a first visit for a toddler.34 In the context of contemporary social media, other platforms, such as Twitter and YouTube, may facilitate awareness of these practice guidelines.
Although profit should not shape clinical decisions, appropriate reimbursement may convince some dentists and hygienists of the usefulness of early dental care, as the absence of reimbursement is a known barrier to caring for young children.11 Providing early visits can be a great practice builder. A specific code for first dental examinations exists in Canada (First Dental Visit/Orientation code 00010), but most providers are likely unaware of this and it is uncertain whether public and government insurance plans accept this code. Advocacy by the CDA and CDHA to promote proper reimbursement can promote its use.
This study is not without limitations. Although a greater response rate from dental hygiene programs was desired, our rate was appropriate and allowed for an environmental scan of dental education in Canada. Response and recall biases are possible, as respondents were asked to estimate the amount of time in their curriculum. Some may have also responded in a particular manner to position their program in a better light.
Conclusions
Many, but not all, dental and dental hygiene programs are teaching students about the recommended age for a first dental visit. It is evident that many graduates are not receiving vital clinical opportunities to assess and manage the oral health needs of infants and toddlers. Dental education should develop innovative ways to expose students to infants and toddlers so that they might respond to the oral health needs of this segment of the population. A broader system-wide approach in dental education can further the oral health agenda of pregnant women and young children.
THE AUTHORS
 |
Dr. Schroth is associate professor, department of preventive dental science, college of dentistry, and departments of pediatrics and child health and community health sciences, college of medicine, faculty of health sciences, University of Manitoba; and research scientist, Children's Hospital Research Institute of Manitoba, Winnipeg, Manitoba. |
 |
Dr. Quiñonez is associate professor, school of dentistry, University of North Carolina. |
 |
Mr. Yaffe is research assistant, college of dentistry, faculty of health sciences, University of Manitoba; dental student, faculty of dentistry, University of Minnesota. |
 |
Ms. Bertone is assistant professor and director school of dental hygiene, college of dentistry, faculty of health sciences, University of Manitoba. |
 |
Dr. Hardwick is in private practice, Nanaimo, British Columbia. |
 |
Dr. Harrison is professor, faculty of dentistry, University of British Columbia. |
Correspondence to: Dr. Robert J. Schroth, Faculty of Health Sciences, Department of Preventive Dental Science (College of Dentistry) and Department of Pediatrics & Child Health (College of Medicine), University of Manitoba, 507—715 McDermot Ave., Winnipeg MB R3E 3P4. Email: umschrot@cc.umanitoba.ca
Acknowledgements
Small-grant funding for this study was provided by the Children's Hospital Research Institute of Manitoba (formerly the Manitoba Institute of Child Health). At the time of this study, RS held a Manitoba Medical Service Foundation/Manitoba Health Research Council Clinical Research Professorship in Population Medicine. AY received a summer studentship from the Children's Hospital Research Institute of Manitoba. We thank Eleonore Kliewer and Jeremy Levi for their assistance with data collection and management and Zachary Goldberg for assistance with survey development.
This article has been peer reviewed.
References
- Nowak AJ, Quiñonez RB. Visionaries or dreamers? The story of infant oral health. Pediatr Dent. 2011;33(2):144-52.
- Early childhood caries (position statement). Ottawa: Canadian Dental Association; 2010. [accessed 2015 Jul 26]. Available: http://www.cda-adc.ca/en/about/position_statements/ecc/
- Policy on early childhood caries (ECC): classifications, consequences, and preventive strategies. Chicago: American Academy of Pediatric Dentistry; 2014. [accessed 2015 Jul 24]. Available: http://www.aapd.org/media/Policies_Guidelines/P_ECCClassifications.pdf
- Committee on Clinical and Scientific Affairs. Report on early childhood caries. Ottawa: Canadian Dental Association; 2010. [accessed 2015 Jul 24]. Available: /sites/default/files/pdf/ccsa/ECC-Report-FINAL-April-2010_for-jcda-website.pdf.
- Lee JY, Bouwens TJ, Savage MF, Vann WF Jr. Examining the cost-effectiveness of early dental visits. Pediatr Dent. 2006;28(2):102-5.
- Stijacic T, Schroth RJ, Lawrence HP. Are Manitoba dentists aware of the recommendation for a first visit to the dentist by age 1 year? J Can Dent Assoc. 2008;74(10):903.
- Schroth RJ, Yaffe AB, Edwards JM, Hai-Santiago K, Ellis M, Moffatt ME, et al. Dentists' views on a province-wide campaign promoting early dental visits for young children. J Can Dent Assoc. 2013;79:d138.
- Savage MF, Lee JY, Kotch JB, Vann WF Jr. Early preventive dental visits: effects on subsequent utilization and costs. Pediatrics. 2004;114(4):e418-23.
- Beil H, Rozier RG, Preisser JS, Stearns SC, Lee JY. Effect of early preventive dental visits on subsequent dental treatment and expenditures. Med Care. 2012;50(9):749-56.
- Pahel BT, Rozier RG, Stearns SC, Quiñonez RB. Effectiveness of preventive dental treatments by physicians for young Medicaid enrollees. Pediatrics. 2011;127(3):e682-9.
- Garg S, Rubin T, Jasek J, Weinstein J, Helburn L, Kaye K. How willing are dentists to treat young children?: a survey of dentists affiliated with Medicaid managed care in New York City, 2010. J Am Dent Assoc. 2013;144(4):416-25.
- Long CM, Quinonez RB, Rozier RG, Kranz AM, Lee JY. Barriers to pediatricians' adherence to American Academy of Pediatrics oral health referral guidelines: North Carolina general dentists' opinions. Pediatr Dent. 2014;36(4):309-15.
- Schroth RJ, Wilson A, Prowse S, Edwards JM, Gojda J, Sarson J, et al. Looking back to move forward: understanding service provider, parent, and caregiver views on early childhood oral health promotion in Manitoba, Canada. Can J Dent Hyg 2014;48:99-108.
- Quinonez RB, Kranz AM, Lewis CW, Barone L, Boulter S, O'Connor KG, et al. Oral health opinions and practices of pediatricians: updated results from a national survey. Acad Pediatr. 2014;14(6):616-23.
- Accreditation requirements for Doctor of Dental Surgery (DDS) or Doctor of Dental Medicine (DMD) programs. Ottawa: Commission on Dental Accreditation of Canada; 2013. [accessed 2015 Jul 24]. Available: https://www.cda-adc.ca/cdacweb/_files/DDSDMDRequirements.doc
- Accreditation requirements for dental hygiene programs. Ottawa: Commission on Dental Accreditation of Canada; 2011. 36 pp. [accessed 2015 Jul 24]. Available: https://www.cda-adc.ca/cdacweb/en/accreditation_requirements/dental_hygiene/
- Search for accredited programs. Ottawa: Commission on Dental Accreditation of Canada; 2014. [accessed 2015 Jul 24]. Available: https://www.cda-adc.ca/cdacweb/en/search_for_accredited_programs/
- Use of fluorides in caries prevention (position statement). Ottawa: Canadian Dental Association; 2012. [accessed 2015 Jul 26]. Available: http://www.cda-adc.ca/en/about/position_statements/fluoride/
- Darmawikarta D, Chen Y, Carsley S, Birken CS, Parkin PC, Schroth RJ, et al. Factors associated with dental care utilization in early childhood. Pediatrics. 2014;133(6):e1594-600.
- First visit to the dentist (position statement). Ottawa: Canadian Dental Association; March 2012. [accessed 2015 Jul 24]. Available: https://www.cda-adc.ca/en/about/position_statements/firstvisit/
- Schroth RJ, Boparai G, Boparai M, Zhang L, Svitlica M, Jacob L et al. Tracking early visits to the dentist: a look at the first 3 years of the manitoba dental association's free first visit program. J Can Dent Assoc. 2015 May;81:f8.
- Long CM, Quinonez RB, Rozier RG, Lee JY. The first dental visit: knowledge, attitudes, and behaviors of North Carolina dentists regarding physician referral guidelines. Pediatr Dent 2012;34:162 (Abstract).
- Hood JG. Service-learning in dental education: meeting needs and challenges. J Dent Educ. 2009;73(4):454-63.
- Weber-Gasparoni K, Kanellis MJ, Qian F. Iowa's public health-based infant oral health program: a decade of experience. J Dent Educ 2010;74(4):363-71.
- Your child's baby teeth and maintaining your child's good dental health. Vancouver: British Columbia Dental Association; 2009. [accessed 2015 Jul 24]. Available: http://www.bcdental.org/ECC/index.html
- Maloney S, Haas R, Keating JL, Molloy E, Jolly B, Sims J, et al. Effectiveness of Web-based versus face-to-face delivery of education in prescription of falls-prevention exercise to health professionals: randomized trial. J Med Internet Res 2011;13(4):e116.
- Seale NS, Casamassimo PS. U.S. predoctoral education in pediatric dentistry: its impact on access to dental care. J Dent Educ. 2003;67(1):23-30.
- Forsetlund L, Bjørndal A, Rashidian A, Jamtvedt G, O'Brien MA, Wolf F, et al. Continuing education meetings and workshops: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009;15;(2):CD003030.
- McFarland TB, Quiñonez RB, Phillips C, Lee J, Chung Y. Provision of preventive oral health services to infants and toddlers: North Carolina general dentists' readiness. J Oral Health Comm Dent. 2013;7(3):140-7.
- Fein JE, Quinonez RB, Phillips C. Introducing infant oral health into dental curricula: a clinical intervention. J Dent Educ. 2009;73(10):1171-7.
- Morgan PJ, Cleave-Hogg D. Comparison between medical students' experience, confidence and competence. Med Educ. 2002;36(6):534-9.
- Seale NS, McWhorter AG, Mouradian WE. Dental education's role in improving children's oral health and access to care. Acad Pediatr. 2009;9(6):440-5.
- Bubna S, Perez-Spiess S, Cernigliaro J, Julliard K. Infant oral health care: beliefs and practices of American Academy of Pediatric Dentistry members. Pediatr Dent. 2012;34(3):203-9.
- Hardwick F. How do I perform a first dental visit for an infant or toddler? [Point of Care]. J Can Dent Assoc. 2009;75(8):577-8.