Abstract
Background:
Despite increasing interest in incorporating courses about the social determinants of health (SDOH) in dental curricula, there is limited knowledge about how ready students feel to address SDOH in their future practice. The purpose of this investigation was to describe dental students’ perceptions of undergraduate learning about SDOH and to explore how prepared they felt to address SDOH in their future practice.
Methods
In this qualitative descriptive investigation, we invited third-year undergraduate dental students from the Faculty of Dental Medicine and Oral Health Sciences of McGill University, Montreal, to participate. Fifteen students took part in face-to-face, qualitative, semi-structured interviews, which were audio-recorded, transcribed verbatim and thematically analyzed.
Results:
The participants reported having taken several courses related to social dentistry and explained that they were ready and willing to identify patients’ SDOH. The participants recognized the importance of understanding people’s oral health-related practices in the context of their social and cultural environments. However, even though they were willing to promote preventive practices tailored to patients’ context of life and were open to participating in charitable community activities, they felt they lacked the necessary skills—and perhaps the motivation—to conduct upstream interventions such as advocacy.
Conclusions:
Current dental education attempts to sensitize future dentists about SDOH may not be enough to sustain effective practice changes. It would be appropriate for dental schools to collectively reflect on how to better train students on this subject.
Keywords
Practice change, dental education, social determinants of health, social dentistry, preventive practices
Introduction
Biopsychosocial approaches to medical education, which aim to go beyond the biological model of disease to address the broader social determinants of health (SDOH), have gained interest over recent decades.1 Defined by the World Health Organization as “the conditions in which people are born, grow, live, work, and age,”2 these determinants include factors such as income, education, housing stability, food security and access to health care services. Models aiming to integrate these psychosocial dimensions into traditional biomedical curricula have emerged, and concepts such as social medicine, structural competency and narrative medicine now represent credible alternative approaches.3-6 These trends also apply to dentistry, with institutions such as the American Dental Association calling for a change in dental education.1,7,8
In Canada, the Association of Canadian Faculties of Dentistry (AFCD) has introduced a framework designed to equip dentists with the skills needed to address patients’ SDOH—such as access to care, socioeconomic status, cultural background and structural barriers—emphasizing the dentist’s role in recognizing and responding to these factors at both individual and population levels.9,10 Similarly, in Europe, dental graduates are expected to focus on promoting health, monitoring interventions and implementing effective care strategies at both community and population levels.11 This approach includes understanding the social context in which patients live and addressing their SDOH, namely through advocacy. Advocacy in this context may include raising awareness about oral health disparities, collaborating with community organizations that serve marginalized populations and engaging in policy discussions aimed at improving access to care.12,13
Despite this growing interest, SDOH are still largely taught as a “grocery list” of factors, an approach yielding limited educational impact.14 Additionally, few empirical studies have examined how dental students perceive current reforms in the undergraduate curriculum or assess their readiness to address the SDOH that will affect their future patients’ health. According to the Merriam-Webster dictionary, “readiness” denotes both a state of preparation and an attitude of prompt willingness. For this study, we defined readiness as referring to undergraduate students’ ability to understand how the SDOH affect health, as well as their perceived competence and positive attitude in addressing these factors in practice. This investigation was guided by the following research question: What are undergraduate dental students’ perceptions of their readiness to address their future patients’ SDOH? More specifically, we aimed to describe undergraduate dental students’ perceptions of undergraduate learning about SDOH and to explore how prepared they felt to address SDOH in their future practice.
Methods
Study Design
We conducted a qualitative descriptive study, a design well suited for summarizing events in clear, everyday language.15 This approach allows researchers to capture the who, what and where of experiences or events, focusing on the basic nature and structure of these occurrences.16 Ethics approval for this study was granted by the McGill Faculty of Medicine and Health Sciences Institutional Review Board (A01-B03-19B).
Participants and Sampling Strategy
Using a purposeful sampling approach,17 we invited all third-year undergraduate dental students enrolled in the Faculty of Dental Medicine and Oral Health Sciences of McGill University, Montreal, during the 2018–19 academic year who had completed a course on SDOH (n = 40). To ensure diversity, we employed maximum variation sampling, selecting participants based on age, sex, and cultural and academic backgrounds. Ultimately, 15 students volunteered to participate in interviews. Following Sandelowski’s guidelines,15,16 this sample size aligns with the recommended range of 12 to 15 participants for qualitative interviews in studies of this type. Once the course on SDOH was complete, including evaluations, we provided students with an overview of the project and sent a consent form by email, outlining the study’s objectives, methods and ethical principles.
Theoretical Framework
This study was guided by competency 5 (Health Promotion) of the ACFD educational framework,9 which emphasizes dentists’ responsibility to address SDOH through advocacy, social justice and ethical practice. Because this competency aligned directly with our study aims, it informed development of the interview guide and provided the basis for deductive coding during data analysis. Figure 1 illustrates the ACFD framework, and Table 1 shows examples of the interview guide questions. [Note: the complete interview guide is available to readers, upon request at: jcda@cda-adc.]
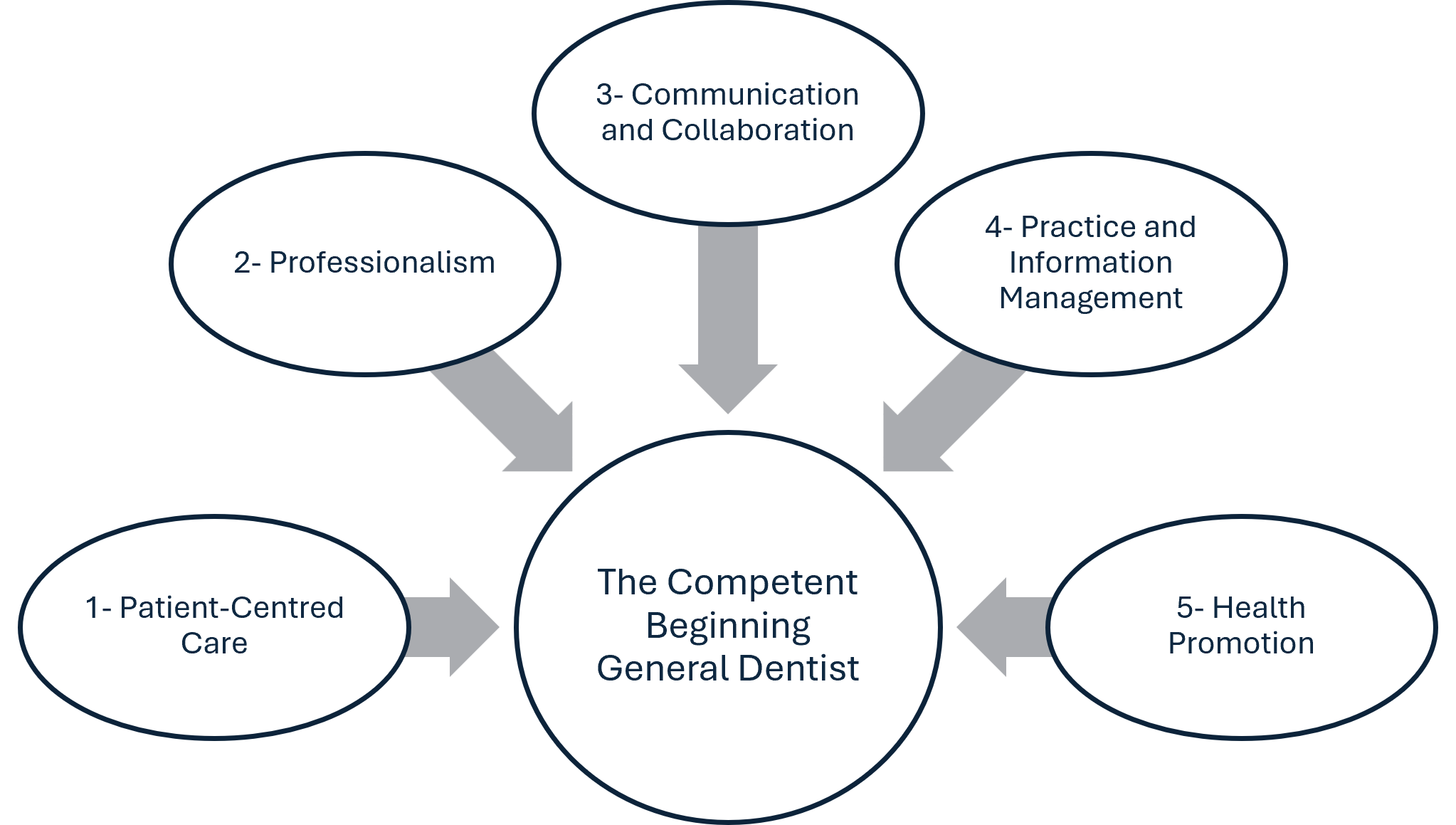
Figure 1: The educational framework of the Association of Canadian Faculties of Dentistry. See: https://acfd.ca/wp-content/uploads/ACFD-Educational-Framework.pdf
|
Main theme |
Sample questions |
|---|---|
| Identifying SDOH | According to you, how pertinent is it to identify patients’ SDOH? Why is or why isn’t it pertinent? |
| How do you think dentists/you could identify their/your patients’ SDOH? | |
| Tackling SDOH | How do you think that you could, in your clinical practice, tackle your patients’ SDOH? |
| How feasible is it to tackle your patients’ SDOH? | |
| Responding to oral health promotion needs of a community | Why do you think that oral health promotion could impact your patient oral health? |
| What resources would you use for the advocacy? |
Data Collection
We gathered data through semi-structured interviews, arranged individually with each participant at a convenient time and place. The first author (N.E.) pilot-tested the questions with a dentist that has graduated, to make sure the questions flowed well and were easy to understand, then conducted interviews with participants in a cafeteria near the Faculty of Dental Medicine and Oral Health Sciences. The researcher (N.E.) first provided a brief overview of the interview process and the study’s purpose and then asked participants for their consent. After reading and signing the consent form, participants introduced themselves and shared demographic information, including their age, sex, birth country and academic background. The interviews were conducted in English during summer and fall 2019, and each interview lasted 20 to 50 minutes.
After each interview, the researcher completed a reflection report to summarize the interview process and highlight key ideas from the conversation. The interviews were audio-recorded digitally, transcribed verbatim and subsequently anonymized and password-protected for secure sharing with the coauthors.
Data Analysis
The first author (N.E.), under the supervision of the second and final authors (C.R., C.B.), initially coded the transcripts using inductive semantic thematic analysis.18 The coding was done manually in Word 365 (Microsoft Corporation, Redmond, WA).19 Emerging themes were then discussed and refined through a series of team meetings. Notably, data analysis was conducted concurrently with fieldwork, and additional interviews were scheduled until thematic saturation20 was reached—around the 13th interview—when no new themes emerged from participant responses. Nonetheless, interviews continued until the 15th participant, at which point data collection was concluded.
Results
The demographic characteristics of the 15 student participants (10 women and 5 men) are summarized in Table 2. Participant age ranged from 22 to 40 (median 25) years. Most of the participants, whether born in Canada or not, were first- or second-generation immigrants. Participants had diverse academic backgrounds before entering dental school. Four had enrolled directly from Quebec’s CEGEP (Collège d'enseignement général et professionnel) system and had been required to complete an additional year in the university’s dental preparatory program. Eight participants held a Bachelor of Science degree, and 3 held degrees in nonscientific fields. Although detailed academic credentials were not collected (to preserve confidentiality), a few participants mentioned additional diplomas or postgraduate training. Just over half of participants (n = 8) planned to work as general practitioners and/or specialists, while smaller numbers intended to pursue residency or specialization (n = 2), join a governmental institution (n = 3) or practice in a developing country (n = 1), with one participant still unsure about their future plans.
Two overarching themes emerged from the analysis: feeling competent in identifying patients’ SDOH and feeling competent in addressing patients’ SDOH.
|
Characteristic |
No. of participants |
|---|---|
|
aCompletion of the university’s dental preparatory program following admission directly from the CEGEP (Collège d’enseignement général et professionnel) system in Quebec. |
|
| Age (years) | |
| 22–24 | 5 |
| 25–26 | 6 |
| 27–29 | 2 |
| ≥ 30 | 2 |
| Sex | |
| Female | 10 |
| Male | 5 |
| Birth country | |
| Canada | 6 |
| Outside of Canada | 9 |
| Prior academic background | |
| Bachelor of Science (including MSc/diploma) | 8 |
| Other bachelor’s degree | 3 |
| Dental preparatory programa | 4 |
| Future practice interest | |
| General practitioner and/or specialist | 8 |
| Residency or specialization | 2 |
| Governmental institution | 3 |
| Practice in a developing country | 1 |
| Unsure | 1 |
Theme 1: Feeling Competent in Identifying Patients’ SDOH
During the interviews, participants expressed confidence in their ability to recognize patients’ SDOH, emphasizing the importance of gathering comprehensive information to provide well-rounded dental care. Although some participants had encountered this concept in the dental program, others were introduced to it earlier, for example, in sociology courses during their undergraduate studies. Those with prior professional degrees also acknowledged that their previous education had deepened their understanding of SDOH and shaped their approach to patient care.
The influence of prior higher education on participants’ awareness of SDOH appeared significant, enhancing their sensitivity to patients’ conditions and life contexts. Some participants, for example, noted how this background made them more aware of both human and societal dimensions in care delivery:
I am a bit biased in that regard because in my first bachelor, it was a major in physiology but a minor in social studies in medicine and I took anthropology, sociology. … It was really helpful to understand about SDOH. (Participant 1)
For these participants, the connections between social conditions, health status and access to health care were evident. They emphasized that their previous education had shifted their perspective from an approach focused on the individual to one that considered social and environmental factors. They added that addressing these broader factors is essential not only for tackling specific dental issues but also for understanding patients’ ability to afford treatment and maintain good oral hygiene and dietary habits.
Participants emphasized the importance of being skilled in identifying patients’ SDOH. They noted that qualities such as empathy and cultural respect are essential for recognizing these factors and felt prepared to gather this information from patients. Additionally, most participants valued having a thorough understanding of patients’ cultures, values and beliefs to better meet their needs and provide appropriate care:
You don’t know maybe that person, have like three people disable to take care of, and the last of the importance is the flossing. … It makes you judgmental but at the same time, the other side of the coin, you have to be aware of which are the determinants of health to be able to provide benefits. (Participant 2)
All participants highlighted the importance of effective communication with patients and the need to invest time during the first appointment to gather as much information as possible. They felt this approach was essential for establishing an accurate diagnosis, developing an appropriate treatment plan and coordinating future appointments:
In a private traditional clinic, what inspired me is the latest family dentist. He takes 10-15 minutes from the first initial appointment out of the dental chair into an office, where is just a desk, face to face and … this is the perfect opportunity to go over some of patients’ limitations, for example financial restraints, and just being open-minded to what the health conditions that they have. (Participant 1)
All participants discussed the uniqueness of each patient’s reality and explained that, through the person-centred approach taught in their third-year courses, they were better able to empathize with patients and understand the roots of their dental issues. They felt this approach enabled them to provide care tailored to each patient’s situation and even to consider broader, upstream interventions:
I think that you have the responsibility to really, like, … engage with the government and policies and everything to try to reach this upstream level. … Like, you have to be the voice of the people, to make those changes happen, because people don’t necessarily know themselves. (Participant 8)
Participants noted that a respectful approach was essential for understanding patients’ beliefs and values, as well as acknowledging that dental care is not always a priority for everyone. They cited examples of how economic circumstances, lifestyle and individual needs could limit people’s ability to maintain oral health. They also observed that without changes in socioeconomic conditions, dental problems would likely persist despite treatment:
If a person is jobless and he is always constantly stressed and binge eating, or he does not have money to buy a toothbrush or toothpaste you know, that eventually leads to caries and no matter how good of fillings you do, yeah it will eventually fail. (Participant 14)
Overall, a recurring theme in the interviews was the importance of exposure to patients from diverse cultures and socioeconomic backgrounds. Participants recognized these experiences as essential for gaining insight into varied realities and providing dental care tailored to each patient’s needs. All participants agreed that this cultural sensitivity should be further strengthened through various courses, clinical rotations and community-based projects.
Theme 2: Feeling Competent in Addressing Patients’ SDOH
At the individual level (i.e., personal interactions with patients), participants felt well prepared and confident in offering preventive dental care, along with advice on diet and oral hygiene to complement surgical and technical procedures. They emphasized prevention as a key aspect of dental treatment and felt comfortable making tailored recommendations that took into account each patient’s unique context and lifestyle.
While operative procedures were a significant part of their training, participants believed that these needed to be paired with “patient education,” effective “oral hygiene instructions” and dietary guidance for best results. However, participants primarily focused on addressing patients’ risk factors and did not discuss implementing broader, upstream interventions.
I can recommend things like, limiting juices and having more water is not too expensive, or, you know, like getting into changing the tooth-brush every couple of months, so they can have more better brushing, or adding nighttime brushing into their sequence [of] events to go to bed, you know. I think those things, it is not expensive to do. (Participant 5)
Most participants expressed a willingness to engage in community-level oral health promotion activities in the future. They recognized the value and impact of charitable work for targeted populations and felt both confident and, to some extent, prepared to participate in these initiatives. All participants noted that their involvement in outreach activities during dental school enhanced their understanding of diverse cultural and social groups, inspiring them to continue such work in their careers. They also highlighted how these experiences taught them to navigate language barriers, interpret body language and respect people with different values and beliefs:
I always have the idea … like, why don’t people get the idea of, instead of paying hygienists or an assistant to show people how to brush, just get [out into] your population? Like, one Saturday morning, you just seat them there and give them fruits or something not cariogenic. ... (Participant 2)
Although some participants expressed a willingness to advocate for individuals lacking access to dental care, others felt uncomfortable with this role, explaining that advocacy did not align with their personality or that they did not feel adequately prepared for it: “Right now, I would not see myself doing that type of stuff, I guess it is just a personality thing” (Participant 14). These participants noted that they planned to focus primarily on clinical work and, if possible, volunteer in community-level oral health promotion activities. However, they all acknowledged the value of advocacy and mentioned they could support it in the future through actions like voting or sharing information within their communities:
Ah, I know that these kinds of things are important, but I do not feel like I’m the right person for this. Like I do not see myself as someone who is going to advocate and make change. That is not my goal, I guess. But I know it is really important to do it, but I do not think that it’s going to be one of my focuses. (Participant 13)
Some participants who were willing to advocate for their patients and communities felt unprepared and unsure about how or at what level to engage effectively: “But I definitely see myself advocating. But to what level? I do not know. Being realistic, I do not know” (Participant 7). Participants also expressed frustration about feeling powerless to address societal issues and fully support their patients. They noted that university outreach dental clinics were often the primary, if not the only, referral option for patients facing financial difficulties. With these clinics operating at limited capacity, it was discouraging for them to see patients placed on long wait lists. They also wondered where they could refer such patients after they graduate:
We have outreach and summer clinic, and we are able to refer our patients as students, dentists to be these different services. Sometimes, I wonder once I graduated, … how that will work, because we do not have these exact tools. (Participant 10)
Beyond advocacy, many participants expressed a more general sense of unpreparedness when it came to addressing SDOH in clinical settings. This included uncertainty about how to support patients facing financial hardship, unfamiliarity with referral pathways to social services and limited exposure to interdisciplinary care models:
I’m not familiar with the resources and I feel like it’s different in every not just country, different provinces, different cities they have a different name for the resource and it’s very complicated for … even for me, I grew up here, I still don’t know what their names are and what their number is. (Participant 14)
Discussion
As health care increasingly embraces person- and people-centred care, there is a growing need to educate health professionals, including those in dentistry, accordingly.21 While reforms in dental education are underway, they remain difficult to implement. The results of this study suggest that after completing coursework in social dentistry, students feel confident in identifying patients’ SDOH—especially economic challenges—and value an understanding of oral health within social and cultural contexts. However, they feel less prepared to act on these determinants, beyond providing preventive care and volunteering in the community, in particular feeling that they lack the skills and confidence to engage in advocacy or other upstream interventions.
Our findings are consistent with previous research showing that dental students often struggle to fully engage with the SDOH. Reis and colleagues22 reported that students tended to view poverty as a distant issue, with responsibility placed on affected individuals or government. Holden and colleagues23 found that students’ understanding of SDOH was partial, shaped by limited curricular exposure, professional attitudes and a social divide between students and underserved communities. Similarly, Chen and colleagues24 observed that while students felt accountable to individual patients, they did not see addressing oral health inequalities as part of their professional role. Furlini and colleagues25 identified significant research gaps in how community-based dental education prepares students to care for underserved populations. Our study contributes to this literature by showing that even after formal instruction, students may still feel unprepared or disempowered to address these determinants in practice.
Various researchers and clinicians have tried to address this gap in dental education. For example, Watt26 was one of the first to advocate for a shift from “biomedical/behavioural downstream” approaches to more “upstream” solutions. More recently, Bedos and colleagues13 encouraged dental faculties to prioritize biopsychosocial approaches, teaching students how to address SDOH. They proposed the Montreal–Toulouse model, which encourages dentists to engage in understanding, decision-making and intervention across individual, community and societal levels. This approach promotes person-centred care, community collaboration and advocacy for systemic change to address broader SDOH.
These calls for “social dentistry” resonate strongly with the social medicine movement,27 which also emphasizes the need to train future clinicians to be “structurally competent” and to address the fundamental causes of their patients’ illnesses. Hansen and Metzl28 observed that “a number of medical schools and teaching hospitals are adopting a structural competency framework in clinical training, following a series of national conferences in 2012 and 2013 on structural competency attended by clinical professionals.” This competency framework has been applied to racial disparities by Metzl and Hansen,27 but also to gender identity by Donald and colleagues.29
Although models of social dentistry have been discussed in the literature, few dental schools have substantially modified their curricula to better prepare students to address SDOH.13 Social dentistry approaches such as the Montreal–Toulouse model represent an important first step in developing dental programs focused on these competencies. However, for 2 reasons, it can be challenging to alter curricula. First, North American dental programs are typically dense—usually encompassing about 200 credits over 4 years—leaving little room for additional courses. Second, there is a shortage of educators and clinicians qualified to champion and integrate these new approaches throughout the curriculum.
These findings indicate that dental education should move beyond raising awareness of SDOH to focus on equipping students with practical skills to address them. Although participants in our study were confident in identifying economic challenges, they tended to recognize financial barriers more readily than nonfinancial factors such as language, transportation, caregiving responsibilities and limited oral health literacy. To address this gap, curricula should integrate structural competency as a longitudinal theme, linked to clinical training and reinforced through experiential learning. Frameworks like the Montreal–Toulouse model can help to operationalize this shift by guiding students to act across individual, community and societal levels. Additionally, dental programs should provide structured opportunities for students to develop advocacy skills and to engage meaningfully with underserved populations. This requires intentional curriculum design and support from educators trained to model and champion these approaches.
Future research could include an environmental scan of dental curricula across Canadian institutions to assess how and to what extent SDOH are taught, in terms of both content and instructional hours. Longitudinal studies could also explore how dental students’ understanding of and engagement with SDOH evolve over time, particularly in relation to clinical experiences and exposure to community-based learning. Additionally, investigating patient perspectives—especially among underserved populations—could offer valuable insights into how socially responsive care is perceived and where gaps remain between training and practice. Together, these lines of inquiry could help inform more comprehensive and effective curricular strategies.
This study had some limitations. It was conducted within the specific context of a Canadian dental school in Montreal. Caution is therefore needed when generalizing these results to different academic settings. Additionally, students’ positive responses toward addressing patients’ social conditions may reflect a social desirability bias or self-selection, as students interested in this topic may have been more likely to participate. Most participants had an immigrant background, which is not surprising given Canada’s status as a country of immigration and given that McGill University includes many international students. The study also had several strengths. The data offer rich insights into dental students’ views on addressing SDOH, an underexplored yet increasingly important area in dental education. Additionally, the use of qualitative methods allowed for in-depth exploration of students’ perspectives, which can inform curriculum development and future research.
Conclusion
This study has highlighted the following key issue in dental training: while current dental education raises awareness about SDOH, it may not be sufficient to drive meaningful changes in practice. Dental schools should therefore consider collectively re-evaluating how to better equip students to address SDOH. Adopting existing biopsychosocial frameworks, such as the Montreal–Toulouse model, and learning from the experiences of medical schools are promising avenues for advancing excellence in contemporary dental education.
THE AUTHORS
 |
Dr. Enriquez is a periodontist, faculty of dental medicine and oral health sciences, McGill University, Montreal, Quebec. |
 |
Dr. Rodriguez is professor in the department of family medicine, school of medicine and institute of health sciences education, faculty of medicine and health sciences, McGill University, Montreal, Quebec. |
 |
Dr. Fathi is a PhD student in the faculty of dental medicine and oral health sciences, McGill University, Montreal, Quebec. |
 |
Dr. Bedos is professor in the faculty of dental medicine and oral health sciences, McGill University, Montreal, Quebec. |
Corresponding author: Dr. Christophe Bedos, Faculty of Dental Medicine and Oral Health Sciences, McGill University, 2001 McGill College Avenue, Suite 500, Montreal, QC H3A 1G1. Email: christophe.bedos1@mcgill.ca
Funding
This study was supported by internal funding from the faculty of dental medicine and oral health sciences, McGill University.
Acknowledgements
The authors express their gratitude to the students who participated in this study and kindly shared their perspectives. Additionally, they thank the people who contributed to the development of this project: Dr. Nora Makansi, for advice during the writing and editing process, and Ellya Farah, a Master’s student who generously collaborated with some of the transcriptions.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- Coria A, McKelvey TG, Charlton P, Woodworth M, Lahey T. The design of a medical school social justice curriculum. Acad Med. 2013;88(10):1442-9. doi: 10.1097/ACM.0b013e3182a325be
- Commission on Social Determinants of Health. Closing the gap in a generation: Health equity through action on the social determinants of health. Final report of the Commission on Social Determinants of Health. Geneva: World Health Organization; 2008. Available: https://www.who.int/initiatives/action-on-the-social-determinants-of-health-for-advancing-equity/world-report-on-social-determinants-of-health-equity/commission-on-social-determinants-of-health (accessed 2026 Mar 30).
- Apelian N, Vergnes JN, Bedos C. Humanizing clinical dentistry through a person-centred model. Int J Whole Person Care. 2014;1(2):30-50. doi: 10.26443/ijwpc.v1i2.2
- Dharamsi S, Ho A, Spadafora SM, Woollard R. The physician as health advocate: Translating the quest for social responsibility into medical education and practice. Acad Med. 2011;86(9):1108-13. doi: 10.1097/ACM.0b013e318226b43b
- Sharma M, Pinto AD, Kumagai AK. Teaching the social determinants of health: A path to equity or a road to nowhere? Acad Med. 2018;93(1):25-30. doi: 10.1097/ACM.0000000000001689
- Ventres W, Dharamsi S. Socially accountable medical education-the REVOLUTIONS framework. Acad Med. 2015;90(12):1728. doi: 10.1097/ACM.0000000000000872
- DePaola DP. The revitalization of U.S. dental education. J Dent Educ. 2008;72(2 Suppl 2):28-42. doi: 10.1002/j.0022-0337.2008.72.2_suppl.tb04476.x
- DePaola DP, Slavkin HC. Reforming dental health professions education: a white paper. J Dent Educ. 2004;68(11):1139-50. PMID: 15520233
- Association of Canadian Faculties of Dentistry. ACFD educational framework for the development of competency in dental programs. Toronto: The Association; 2016. Available: https://acfd.ca/wp-content/uploads/ACFD-Educational-Framework.pdf (accessed 2026 Mar 30).
- Feldman CA, Valachovic RW. Renewing our commitment to the future of dental education: ADEA CCI 2.0 [editorial]. J Dent Educ. 2017;81(3):259-61. doi: 10.1002/j.0022-0337.2017.81.3.tb06269.x
- Gallagher J, Field JC. The graduating European dentist—domain IV: Dentistry in society. Eur J Dent Educ.2017;21(Suppl 1):25-7. doi: 10.1111/eje.12311
- Bedos C, Apelian N, Vergnes JN. Social dentistry: An old heritage for a new professional approach. Br Dent J. 2018;225(4):357-62. doi: 10.1038/sj.bdj.2018.648
- Bedos C, Apelian N, Vergnes JN. Towards a biopsychosocial approach in dentistry: The Montreal–Toulouse model. Br Dent J. 2020;228(6):465-8. doi: 10.1038/s41415-020-1368-2
- Donoff RB. It is time for a new Gies report. J Dent Educ. 2006;70(8):809-19. PMID: 16896083
- Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334-40. doi: 10.1002/1098-240X(200008)23:4<334::AID-NUR9>3.0.CO;2-G
- Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33(1):77-84. doi: 10.1002/nur.20362
- Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179-83. doi: 10.1002/nur.4770180211.
- Clarke V, Braun V. Thematic analysis. J Posit Psychol. 2017;12(3):297-8. doi: 10.1080/17439760.2016.1262613
- Adu P. Manually assigning codes to data. In: A step-by-step guide to qualitative data coding. New York: Routledge; 2019. Available: https://search.ebscohost.com/login.aspx?direct=true&scope=site&db=nlebk&db=nlabk&AN=2097761 (accessed 2025 Aug 1).
- Patton MQ. Qualitative research and evaluation methods : integrating theory and practice. 4th ed. Thousand Oaks (CA): Sage Publications, Inc.; 2015.
- Sabato E, Owens J, Mauro AM, Findley P, Lamba S, Fenesy K. Integrating social determinants of health into dental curricula: An interprofessional approach. J Dent Educ. 2018;82(3):237-45. doi: 10.21815/jde.018.022
- Reis CMR, Rodriguez C, Macaulay AC, Bedos C. Dental students’ perceptions of and attitudes about poverty: A Canadian participatory case study. J Dent Educ. 2014;78(12):1604-14. PMID: 25480275
- Holden ACL, Leadbeatter D. Conceptualisations of the social determinants of health among first‐year dental students. BMC Med Educ. 2021;21:164. doi: 10.1186/s12909-021-02602-1
- Chen V, Foster Page L, McMillan J, Lyons K, Gibson B. Measuring the attitudes of dental students towards social accountability following dental education—Qualitative findings. Med Teach. 2016;38(6):599-606. doi: 10.3109/0142159X.2015.1060303
- Furlini L, Noushi N, Castonguay G, Allison P, Bedos C, De Souza R, et al. Assessing dental students’ readiness to treat populations that are underserved: A scoping review. J Dent Educ. 2018;82(5):483-91. doi: 10.21815/JDE.018.053
- Watt RG. From victim blaming to upstream action: tackling the social determinants of oral health inequalities. Community Dent Oral Epidemiol. 2007;35(1):1-11. doi: 10.1111/j.1600-0528.2007.00348.x
- Metzl JM, Hansen H. Structural competency: theorizing a new medical engagement with stigma and inequality. Soc Sci Med. 2014;103:126-33. doi: 10.1016/j.socscimed.2013.06.032
- Hansen H, Metzl J. Structural competency in the U.S. healthcare crisis: Putting social and policy interventions into clinical practice. J Bioeth Inq. 2016;13(2):179-83. doi: 10.1007/s11673-016-9719-z
- Donald CA, DasGupta S, Metzl JM, Eckstrand KL. Queer frontiers in medicine: A structural competency approach. Acad Med. 2017;92(3):345-50. doi: 10.1097/ACM.0000000000001533