Abstract
Background:
Medical–dental integration (MDI) is increasingly recognized as a promising approach to preventing disease and reducing oral health disparities. Although integrated care delivery is central to community health centres (CHCs), limited knowledge exists on how CHCs in British Columbia integrate medical and dental services. We conducted an environmental scan with the aim of describing the current state of MDI practices and strategies employed by CHCs in British Columbia.
Methods
A cross-sectional environmental scan approach combining passive conditioned viewing and active searching modes was used. Data were collected through an Internet search of organizational materials, an online survey of CHC representatives and clarifying telephone conversations. We included BC CHCs that addressed oral health through referrals or direct service provision. Descriptive statistical and content analyses were conducted. MDI practices and strategies were categorized as relating to workforce, information sharing, evidence-based care, and measuring and monitoring.
Results:
Among the 23 CHCs included in the study, approximately half provided on-site dental services through co-located clinics (n = 9, 39%) or embedded dental hygienists (n = 3, 13%), whereas others relied on referrals (n = 9, 39%), and a smaller subset (n = 2, 9%) partnered with local private and nonprofit dental practices to provide off-site care. Implementation of integrating processes was limited overall. Less than one-quarter of the CHCs reported processes for information exchange, referral tracking and standardized screening protocols. Few reported using dedicated personnel, training resources or interoperable technology to support integration.
Conclusions:
Our findings established a baseline understanding of MDI in BC CHCs, revealing significant gaps in the implementation of integrating processes. Further research is needed to explore these gaps and to build on lessons learned from other jurisdictions.
Keywords
Medical–dental integration, integrated delivery of health care, community health services, dental health services, primary health care
Introduction
Oral health is an integral component of overall health,1-3 yet the dental and medical professions have traditionally operated in silos in many countries, including Canada.1 This division has perpetuated gaps in shared understanding and interprofessional collaborative practice4 and has also placed an undue burden on individuals who are disproportionately affected by systemic barriers that impede access to services.5 Globally, a higher burden of oral disease affects structurally vulnerable groups, including individuals living in poverty, older adults, children, people living in remote and rural communities, refugees, people living with disabilities, and people from minority and/or other socially marginalized groups.1,6
In Canada and internationally,7,8 there are growing calls to redesign health services, specifically by integrating dental and medical care, to reduce the burden of oral diseases and improve access to oral health care.1,8 Medical–dental integration (MDI) has been advocated as a promising way to address oral health inequities, to improve health outcomes and the experiences of patients and providers, and to realize cost savings.9,10 MDI is an approach to care that incorporates oral health services into primary care and behavioural health,11 aiming to improve processes and outcomes through enhanced accessibility, coordination and continuity of care.12,13 Common approaches to MDI include coordinating care,4 employing interdisciplinary networks and teams,9 and physically co-locating dental services in primary care settings such as community health centres (CHCs).13
CHCs are nonprofit, multisectoral, community-governed health organizations that deliver integrated health care and social services. These organizations are committed to providing comprehensive, accessible, affordable and culturally appropriate team-based services to communities that experience systemic barriers to care.14,15 CHCs often serve the members of structurally vulnerable populations, who may present with multiple medical comorbidities complicated by unmet social needs,14 thus providing an opportunity to unify care silos in support of comprehensive care.16
Although there is growing understanding of the need for an integrated approach to oral health care, there is also limited practical guidance and understanding of how to actually integrate these services.9,17 In addition, most documented MDI initiatives are based in the United States,9 with limited generalizability to the Canadian context. In British Columbia, CHCs already integrate primary care and public health functions,18 making them promising settings for exploring collaboration. However, there is no comprehensive understanding of existing MDI initiatives in BC CHCs, so it is unclear which and to what extent services are integrated. Understanding the strategies that CHCs use to integrate medical and dental services is crucial for informing future programs and policy development.
To bridge this gap, we conducted an environmental scan of MDI initiatives within CHCs in British Columbia to better understand the landscape in terms of current programs and activities. The objective was to identify and describe the existing state of practices and strategies employed by BC CHCs in their efforts to integrate medical and dental services.
Methods
A cross-sectional environmental scan approach was selected as an appropriate method to systematically gather and synthesize information on the types and scope of practices and strategies used by BC CHCs to integrate medical and dental services. This environmental scan represents an initial evidence-mapping phase within a larger, multiphase research program on MDI in BC CHCs. This methodological approach was selected due to its suitability and utility for describing service landscapes, identifying emerging trends, and informing strategic planning and program development in health care.19 For the context of health services delivery research, Charlton and colleagues20 proposed the following working definition of an environmental scan: “a type of inquiry that involves the collection and synthesis of existing information and/or the pursuit of new evidence to inform decision-making and help shape future response(s) to existing and emerging policy and service delivery issues and opportunities” (p. 7).
Guided by this framing, our environmental scan applied 2 scanning modes from Choo’s model21—conditioned viewing and searching—to capture both passive and active forms of information gathering.19 The conditioned viewing mode involved passive, nonintrusive review of publicly available organizational materials, whereas the searching mode entailed active data collection through an online survey and clarifying telephone conversations with CHC representatives. Together, these approaches aimed to capture both the formal documentation of CHCs and the less visible integration practices in daily operations to provide a foundational overview of how MDI is currently evolving within British Columbia’s community health sector.
Ethics approval
Ethics approval was obtained from the University of British Columbia Behavioural Research Ethics Board (H22-00832). Informed consent was obtained from all participants. To protect confidentiality, identifying details of participating CHCs are not reported, even where such information was publicly accessible.
Inclusion criteria
Eligible CHCs were those registered with the British Columbia Association of Community Health Centres (BCACHC) by August 2024 that were operational, provided primary care services and addressed oral health by direct service provision or referrals. Organizations that had no publicly available information on oral health care provision and that were unable or unwilling to provide details upon request were excluded from the analysis.
Data collection
Once eligible CHCs were identified for inclusion, information on their MDI practices and strategies were sourced in 3 ways. First, online searches were conducted using Google and Yahoo search engines with a combination of the included CHC’s name and various keywords, including “medical dental services BC,” “integrated medical dental” and “dental clinic.” We systematically explored embedded links, downloadable files and related resources from official websites and auxiliary documents. The initial search was completed in September 2023 and updated in August 2024.
Second, an online survey was administered to representatives of the identified CHCs using Qualtrics software (Qualtrics, Provo, UT). Key informant sampling was used to target individuals with expertise on service integration at their respective organizations.22 A BCACHC administrator identified and contacted participants by email to invite participation and provide an information letter outlining the study’s purpose, its voluntary nature and data confidentiality measures. All collected data were deidentified and stored securely on encrypted, access-restricted servers available only to the research team.
The survey was distributed once on February 8, 2024, and responses were collected until April 29, 2024, with reminders sent at 3-week intervals. The survey included closed and open-ended questions about the CHC, the types and scope of health care services and providers, and the integration of practices and processes. Survey items were adapted from previous published surveys assessing MDI23,24 and CHC characteristics.25 Questions were also developed using a modified version of the MDI framework of Gupta and colleagues,17 which outlines key practices and processes for integrating oral health into medical settings, with further details available in their article. We adapted the framework components to capture perspectives of bilateral integration (i.e., integrating dental care within medical practices and vice versa).26 The survey was pilot-tested with CHC administrators (n = 2), medical and dental providers (n = 3) and non–health care professionals (n = 2) for readability and to ensure these aspects were adequate. Pilot responses informed minor modifications to the survey for clarity and were excluded from the final data set. The full survey instrument is available upon request to the JCDA editorial office.
Third, informal telephone conversations were conducted between April 22 and May 14, 2024, to clarify missing or unclear information from the online search and survey. CHC representatives (executive directors, administrators and staff) were contacted using publicly listed phone numbers or those voluntarily provided by survey respondents. Participants in the phone calls answered binary (yes/no) and brief descriptive questions aligned with those asked in the survey. There was no attempt to audio-record the telephone conversations.
Data analysis
All data were collated in an Excel spreadsheet (2024 version; Microsoft Corporation, Redmond, WA) and classified into the following 3 broad categories:
- descriptive information, including the duration of operation and the target population
- provision of medical and dental services, including the oral health care practice model used, the services provided, workforce composition, and service fee and funding structures
- MDI practices and strategies, including the processes and practices implemented across 4 MDI framework categories (dental/medical workforce, information sharing, evidence-based care, and measuring and monitoring)
Descriptive statistics with frequency percentages were used to summarize quantitative data, whereas content analysis to identify common categories was conducted for open-ended items.
Results
The BCACHC has 43 registered members, of which 23 were included in the study. The other 20 were excluded because they were nonoperational (n = 10), did not offer primary care services (n = 4) or did not address oral health in any form (n = 5) or because information about services and practices was lacking (n = 1).
Descriptive information about CHCs
Table 1 summarizes the operational duration and target populations of the CHCs. Just over half had been operational for more than a decade, but almost a quarter were newly established. The CHCs were situated in urban (n = 13, 56%), rural (n = 8, 35%) or mixed (n = 2, 9%) geographic locations across multiple jurisdictions in British Columbia, including the Fraser Health, Interior Health, Island Health, Northern Health and Vancouver Coastal Health regions. The CHCs targeted a range of structurally vulnerable populations but primarily focused on serving people with complex needs (n = 17, 74%), low-income groups (n = 14, 61%) and geographically defined communities (n = 14, 61%). About half of the CHCs additionally reported targeting other population groups (n = 12, 52%), including those affected by infectious diseases, Indigenous communities, LGBTQ2+ individuals, people living with substance use and mental health challenges, migrant farm workers and sex workers.
|
Characteristic |
No. (%) of CHCs |
|---|---|
|
aMultiple responses allowed. |
|
| Duration of operations (years) | |
| < 2 | 5 (22) |
| 2–5 | 3 (13) |
| 6–10 | 3 (13) |
| > 10 | 12 (52) |
| Target populationa | |
| Geographically defined | 14 (61) |
| Children/youth | 11 (48) |
| Pregnant women/new mothers | 11 (48) |
| Seniors | 13 (56) |
| Complex needs | 17 (74) |
| Low income | 14 (61) |
| Unhoused | 10 (43) |
| Newcomers/refugees | 8 (35) |
| Other | 12 (52) |
| Geography | |
| Urban | 13 (56) |
| Rural | 8 (35) |
| Mixed urban and rural | 2 (9) |
Provision of medical and dental services
The types of services and providers available in the CHCs are outlined in Table 2. The majority provided mental health services (n = 17, 74%), community health navigation (n = 13, 56%) and chronic disease management (n = 12, 52%), in addition to primary care (n = 23, 100%). All of the CHCs employed physicians, with frequent involvement of allied health professionals, including registered nurses (n = 18, 78%), nurse practitioners (n = 13, 56%), social workers (n = 14, 61%), clinical counsellors (n = 12, 52%) and community health workers (n = 12, 52%).
|
Characteristic |
No. (%) of CHCs |
|---|---|
|
aFor the 14 community health centres with provision of dental services on site (n = 12) or off site (n = 2). Excludes the 9 community health centres that provided only referrals. |
|
| Medical services | n = 23 |
| Primary care services / general medicine | 23 (100) |
| Pediatrics | 6 (26) |
| Obstetrics and gynecology | 5 (22) |
| Pharmacy | 5 (22) |
| Nutrition counselling / dietician services | 6 (26) |
| Physical therapy, rehabilitation, medical exercise services | 7 (30) |
| Mental health services | 17 (74) |
| Chronic disease management | 12 (52) |
| Community health navigation | 13 (56) |
| Medical providers | n = 23 |
| Physician | 23 (100) |
| Nurse practitioner | 13 (56) |
| Registered nurse | 18 (78) |
| Licensed practical nurse | 6 (26) |
| Pharmacist | 7 (30) |
| Dietician | 6 (26) |
| Physical therapist | 4 (17) |
| Occupational therapist | 3 (13) |
| Kinesiologist | 2 (9) |
| Registered clinical counsellor | 12 (52) |
| Registered psychologist | 2 (9) |
| Social worker | 14 (61) |
| Community health worker | 12 (52) |
| Specialist care | 5 (22) |
| Location of dental services provision | n = 23 |
| Dental services provided on site | 12 (52) |
| Co-located dental clinic | 9 (39) |
| Service partnership with public health dental hygienist | 3 (13) |
| Dental services provided off site | 2 (9) |
| Co-operative managed dental services | 1 (4) |
| Service partnership with local dental clinic | 1 (4) |
| Referrals only | 9 (39) |
| Dental servicesa | n = 14 |
| Examinations | 12 (86) |
| Cleanings and preventive services (e.g., fluoride, sealants) | 12 (86) |
| Basic dentistry services (e.g., fillings, root canals, extractions) | 11 (79) |
| Prosthodontics (e.g., crowns, bridges, dentures) | 7 (50) |
| Orthodontics | 5 (36) |
| Emergency dental care | 11 (79) |
| Dental providersa | n = 14 |
| Dentist | 11 (79) |
| Dental hygienist | 14 (100) |
| Dental assistant | 10 (71) |
| Dental therapist | 0 (0) |
| Other | 5 (36) |
| Dental feesa | n = 14 |
| Discounted dental services | 6 (43) |
| Additional subsidies for eligible clients | 3 (21) |
| No-cost preventive dental services | 3 (21) |
| Funding for dental service provisiona | n = 14 |
| Dental patient fees | 8 (57) |
| Grants | 8 (57) |
| Private donations | 4 (29) |
| Local fundraising | 1 (7) |
About half of the 23 CHCs provided on-site dental services (n = 12, 52%) through co-located dental clinics (n = 9, 39%) or service partnerships with dental hygienists employed by public health authorities (n = 3, 13%), whereas fewer provided off-site care through local dental clinics (n = 2, 9%). A considerable proportion relied on referrals to address clients’ oral health needs (n = 9, 39%). All of the 14 CHCs providing dental services worked with dental hygienists (n = 14, 100%), and the majority worked with dentists (n = 11, 79%). None of these 14 organizations indicated working with a dental therapist, although some (n = 5, 36%) incorporated other dental professionals, including denturists and students from educational institutions. The types of oral health care services provided encompassed preventive, restorative and emergency services.
Among the 14 CHCs providing on-site or off-site dental care, several offered discounted dental services (n = 6, 43%), including additional subsidies to low-income individuals without insurance (n = 3, 21%). A few CHCs provided no-cost preventive dental services (n = 3, 21%), through public health fluoride varnish programs (n = 2) and BC Medical Service Plan coverage for persons with disabilities (n = 1). Funding for dental service provision was primarily sourced from dental patient fees (n = 8, 57%), grants (n = 8, 57%), private donations (n = 4, 29%) and local fundraising (n = 1, 7%).
Implementation of MDI processes and practices
Of the 23 CHCs included in the study, 6 did not provide responses for items related to MDI practices and processes; therefore, percentages reported in the following subsections are based on the 17 CHCs that reported data.
Dental and medical workforce
Figure 1 and Figure 2 illustrate the 6 workforce practices and processes reported by the 17 CHCs included in this part of the analysis. Provision for medical-to-dental referrals (n = 11, 65%) was more common than for dental-to-medical referrals (n = 6, 35%), but evidence of information exchange from medical to dental teams or from dental to medical teams was limited (n = 7, 41%, and n = 3, 18%, respectively). Few CHCs reported dedicated personnel to coordinate dental referrals (n = 2, 12%) or embedded dental providers in medical settings (n = 2, 12%), and no organizations reported dedicated personnel to coordinate medical referrals or embedded other health care providers in dental settings. The use of interprofessional consultations and training resources to support interprofessional practice was nearly absent.
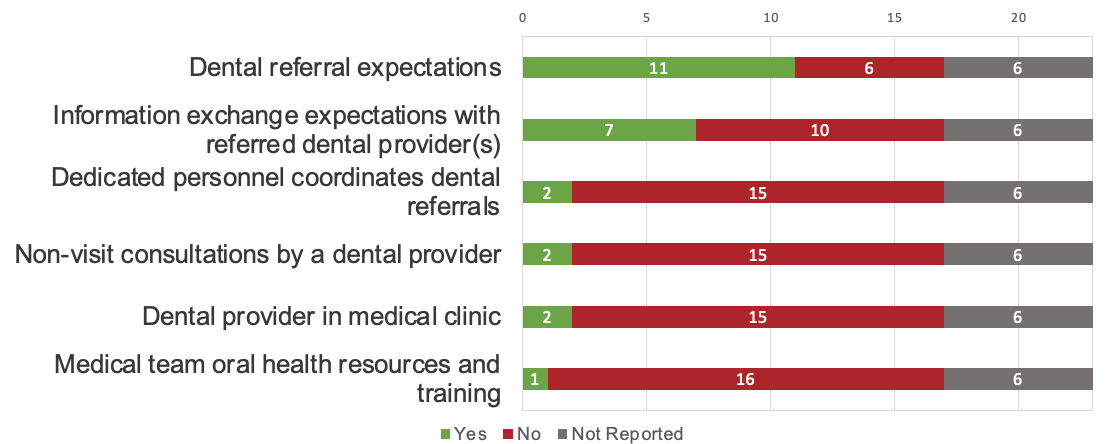
Figure 1: Oral health workforce strategies implemented by community health centres.
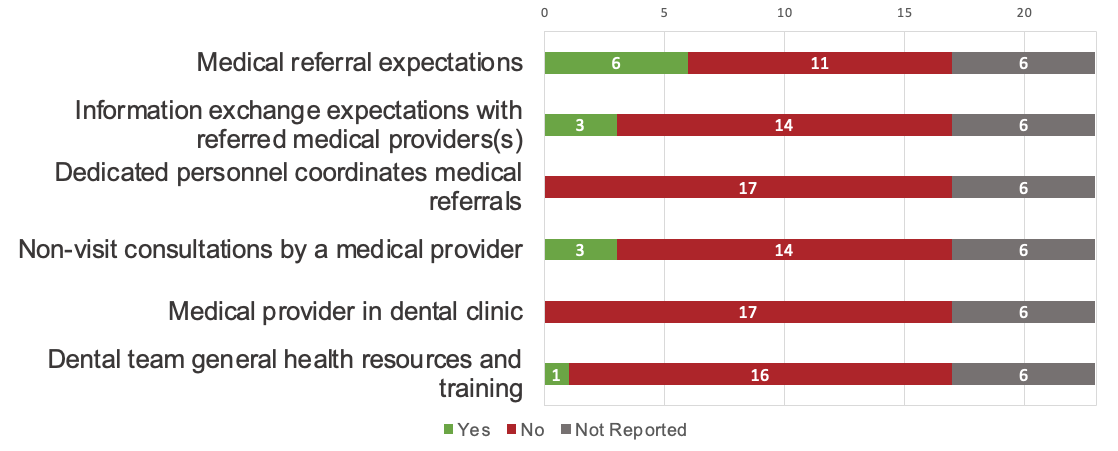
Figure 2: Medical workforce strategies implemented by community health centres.
Information sharing
Figure 3 displays the number of programs that reported implementing information-sharing activities between medical and dental teams. Few CHCs reported formal protocols for information exchange between medical and dental teams (n = 4, 24%). The reported implementation of processes for tracking referrals was also limited. A small proportion of CHCs reported monitoring dental referrals from the medical team (n = 4, 24%), but fewer reported monitoring medical referrals from the dental team (n = 2, 12%). Few CHCs reported having interoperable electronic health records (EHRs) or processes for coordinating medical and dental care appointments (n = 2, 12% for each).
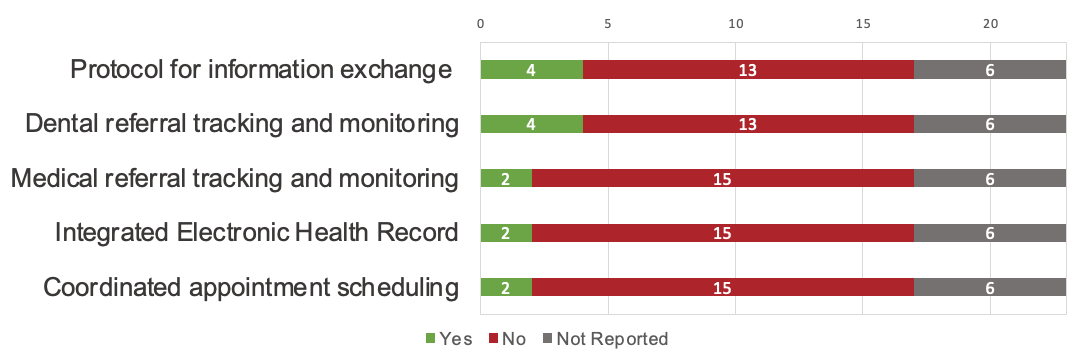
Figure 3: Information sharing strategies implemented by community health centres.
Evidence-based care
Figure 4 illustrates the reported implementation of evidence-based care activities across the CHCs. The use of standardized tools for assessments and evidence-based guidelines was limited overall, and respondents did not necessarily describe the tools as being evidence-based. Four CHCs (24%) reported using a standardized tool for general health screening in the dental setting through the medical history form (n = 3) or during blood pressure screening (n = 1), whereas 2 (12%) reported using a standardized tool for oral health screening in the medical setting, both of which were caries risk assessment tools. Only one CHC (6%) reported using decision support tools to guide medical or dental teams about when to make referrals or seek consultations.
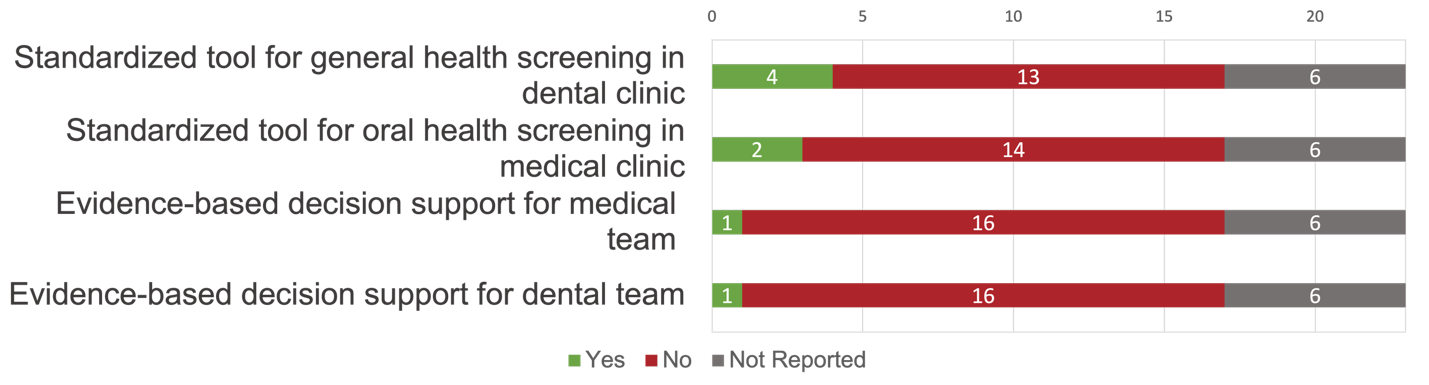
Figure 4: Evidence-based care strategies implemented by community health centres.
Measuring and monitoring
Figure 5 shows the number of programs that reported implementation of various measuring and monitoring processes and practices. Several CHCs reported using quality measures (e.g., client satisfaction surveys) to monitor medical care performance and to understand the outcomes of medical services provided (n = 8, 47%). However, few sites reported similar processes for tracking and improvement of dental care quality (n = 2, 12%). Quality measures and goals were not necessarily aligned or formally adopted, and medical and dental service provision was generally assessed separately. A siloed approach was also reflected in the limited number of CHCs reporting processes for medical providers to monitor and assess symptoms of oral health (n = 5, 29%) and for dental providers to monitor and assess symptoms of general health (n = 3, 18%) over time.
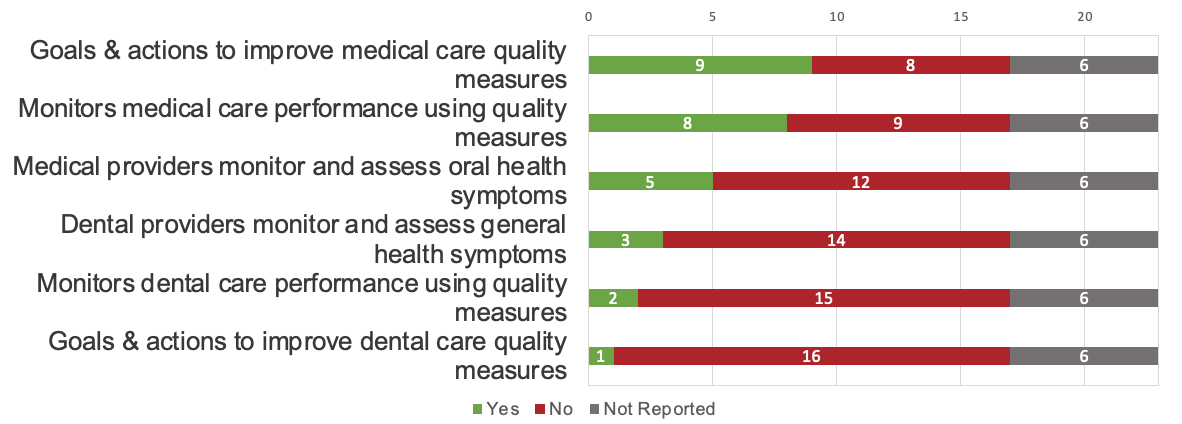
Figure 5: Measuring and monitoring strategies implemented by community health centres.
Discussion
To our knowledge, this environmental scan is the first to provide an overview of MDI initiatives in BC CHCs and to describe the existing state of practices and strategies used to integrate medical and dental services. Our findings show that while many CHCs have taken steps to incorporate oral health into their practice models, few have been able to implement integrating processes that foster interprofessional collaboration or coordinate care holistically. These findings illustrate that MDI within BC CHCs remains to be fully developed. This study establishes a foundational baseline from which to monitor progress of MDI efforts and highlights a structured framework that can be used to enhance understanding and advancement of practices that support integration.
Our findings show that MDI remains emergent, with just over half of the CHCs having some form of MDI. The CHCs predominantly used co-location models to provide dental services through on-site dental clinics or embedded dental hygienists, which is consistent with research on MDI programs in the United States.13,23 Co-location models, which use common resources and infrastructure to coordinate medical and dental care in a shared physical space, have been shown to improve access to referrals and reduce barriers to access more generally.13 However, co-location alone does not ensure integration.24 It is an enabler for interdisciplinary coordinated care27 and bidirectional referral mechanisms,13,23 but our scan found limited evidence of structured processes to support care coordination. Few CHCs with co-located services reported systems for coordinating care appointments or using interoperable EHRs. These findings reflect ongoing challenges, including the lack of shared protocols and systems for effective communication between medical and dental providers.27,28
Moreover, because co-location requires substantial investments in infrastructure, personnel and administrative support,29 a large portion of CHCs in this study used referral models and off-site approaches to address oral health. Such approaches can perpetuate access barriers and contribute to unmet oral health needs.29 Effective communication and collaboration among medical and dental providers is critical for closing the referral loop and supporting positive patient outcomes.13 However, less than one-quarter of the CHCs had established processes for such communication and collaboration. These findings align with those of Harnagea and colleagues,27 who found that unstructured mechanisms for referrals and care coordination were major barriers to integration. Similarly, few CHCs reported using standardized screening tools to support referrals or had implemented processes for interdisciplinary health assessment and monitoring.9,28
Having an interoperable EHR to facilitate care coordination and data sharing is key for MDI but is also one of the most challenging processes to implement.13 Currently, most dental and medical EHRs are not interoperable because they are created and managed separately and use distinct procedural codes.28 The use of “smart phrases” (i.e., trackable text phrases) for documentation and the involvement of referral coordinators have been recommended.13 However, our scan revealed that few CHCs had dedicated personnel or systems to monitor referrals or shared service outcomes. These findings reflect ongoing human resource challenges27 and the lack of formal systems to assess MDI efforts.4,17
An environmental scan in the United States found that well-developed MDI programs included formalized clinical protocols for screening and referral, standardized training, and EHR systems that facilitate and track outcomes.23 Our scan has highlighted significant gaps in these areas for BC CHCs. Studies have also shown that several MDI programs have successfully focused on reducing barriers and enhancing health outcomes in vulnerable population groups, including children, older adults, pregnant women and individuals who need chronic disease management.10,13 The overlap between these groups and those served by BC CHCs suggests a potential opportunity to adapt MDI models to the local context, accounting for the unique socioeconomic and policy environments in which BC CHCs operate.9
Unlike other jurisdictions in North America, such as the United States and Ontario, where CHCs have been scaled up significantly, British Columbia has historically had limited policy-level backing to advance this practice model.30 However, a recent commitment from the BC provincial government to support and fund CHCs as part of broader primary care reforms is encouraging.31,32 Notably, we found that a significant proportion of registered CHCs in BC were newly established or emerging. The evolving landscape of British Columbia’s CHC model may partially explain the variation in dental practice models and the gaps in integration observed in this study. Although oral health services are an important component of primary care, their integration within primary health care settings poses challenges.33 Research underscores the importance of supportive policies and resource allocation for successful integration.27 For instance, in the United States, Federally Qualified Health Centers have been recognized as leaders in this area,34 with approximately 80% providing dental services.35 These centres receive federal funding to ensure access to preventive dental services for underserved populations.35 In contrast, BC CHCs operate without similar mandates or funding structures for dental service provision. Nonetheless, the recently introduced Canadian Dental Care Plan36 is promising, given that the majority of CHCs already provide dental services.
Limitations and strengths
This study collected data through online searches, a survey and clarifying telephone conversations. Despite efforts to discover all resources, some MDI practices and strategies may not have been identified. Approximately one-quarter of the identified organizations could not be reached to verify website information, and CHCs not registered with the BCACHC or lacking publicly available information were excluded. Because the findings were reported in aggregate, site-specific contextual nuances may not be fully represented. This study used a descriptive cross-sectional design to capture MDI practices and processes but did not assess their implementation, outcomes or impact, nor did it seek patients’ perspectives. Longitudinal research is needed to assess these dimensions of BC CHCs.
Despite these limitations, this study offers new insight into the current state of MDI in BC CHCs and establishes a baseline for monitoring progress over time. Using a systematic, multisource approach, this scan identified emerging integration models that are not yet reflected in the Canadian evidence base. The study design and survey tool may be adapted for use in other provinces and support a coordinated understanding of MDI in CHCs nationally. Engagement with CHC stakeholders strengthened the interpretation and practical relevance of the findings, and this engagement will continue through subsequent phases of this research program and ongoing knowledge mobilization activities. Results will be shared directly with participating CHCs and disseminated more broadly through the BCACHC newsletter. Although it was not designed as participatory research, this scan incorporated collaborative engagement and feedback processes that enhance the applicability of results and can inform strategies for advancing MDI implementation across community health settings.
Participating CHCs confirmed many of the identified gaps and noted that completing the survey prompted reflection on potential integration strategies and challenges, including limited funding, limited EHR interoperability and workforce shortages—areas that warrant deeper exploration. Future phases of this research will build on these findings, in particular through a case study at one participating CHC to examine integration processes in greater depth. This work will be conducted in collaboration with a stakeholder implementation advisory group composed of community members, care providers and administrators. These ongoing knowledge mobilization activities and partnerships aim to ensure that findings are discussed, contextualized and translated into practical strategies to support MDI development across community health settings.
Conclusion
This study provides a snapshot of the current landscape of MDI within BC CHCs. Although strides have been made toward incorporating oral health into the CHC practice model, significant gaps remain. The findings are intended to inform organizational stakeholders, policy-makers and researchers about existing programs and practices that encourage coordination and integration, as well as current gaps in MDI implementation, with the hope that this knowledge will in turn inform future practice and policy development. Integrating dental services within CHCs has the potential to improve patients’ access to care, continuity of care once accessed, and oral and systemic health. Further research is needed to bridge the identified gaps and build on the lessons learned from other jurisdictions to advance integrated health service delivery.
THE AUTHORS
 |
Ms. Howey is a PhD Candidate, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. |
 |
Dr. Yoon is associate professor, faculty of medicine and dentistry, University of Alberta, Edmonton, Alberta. |
 |
Dr. Brondani is professor, department of oral health sciences, faculty of dentistry, University of British Columbia, Vancouver, British Columbia. |
 |
Dr. Wallace is professor, school of social work, University of Victoria, Victoria, British Columbia. |
 |
Dr. Bedos is professor, faculty of dental medicine and oral health sciences, McGill University, Montreal, Quebec. |
 |
Dr. Donnelly is associate professor, faculty of dentistry, The University of British Columbia, Vancouver, British Columbia. |
Corresponding author: Madison Howey, 384-2199 Westbrook Mall, Vancouver, BC, V6T 1Z3. Email: mlhowey@dentistry.ubc.ca
Funding
Funding for Madison Howey’s doctoral stipend, in support of this work, was provided by GreenShield Cares Canada
Acknowledgements
This work was supported by GreenShield Cares Canada. The authors thank the administrative team of the British Columbia Association of Community Health Centres for their support in identifying participants, administering the survey and disseminating findings to stakeholders. The authors also thank the individuals who piloted the survey instrument for their time and valuable feedback.
The authors have no declared financial interests.
This article has been peer reviewed.
References
- World Health Organization. Global oral health status report: towards universal health coverage for oral health by 2030. Geneva (Switzerland): The Organization; 2022. Available: https://www.who.int/publications/i/item/9789240061484 (accessed 2023 May 10).
- Seitz MW, Listl S, Bartols A, Schubert I, Blaschke K, Haux C, et al. Current knowledge on correlations between highly prevalent dental conditions and chronic diseases: an umbrella review. Prev Chronic Dis. 2019;16:E132. doi: 10.5888/pcd16.180641
- Kisely S, Baghaie H, Lalloo R, Siskind D, Johnson NW. A systematic review and meta-analysis of the association between poor oral health and severe mental illness. Psychosom Med. 2015;77(1):83-92. doi: 10.1097/PSY.0000000000000135
- Atchison KA, Rozier RG, Weintraub JA. Integration of oral health and primary care: communication, coordination and referral [commentary]. NAM Perspect. 2018;1-12. doi: 10.31478/201810e
- Northridge ME, Kumar A, Kaur R. Disparities in access to oral health care. Annu Rev Public Health. 2020;41:513-35. doi: 10.1146/annurev-publhealth-040119-094318
- Petersen PE. Strengthening of oral health systems: oral health through primary health care. Med Princ Pract. 2014;23 (Suppl 1):3-9. doi: 10.1159/000356937
- Farmer J, Singhal S, Ghoneim A, Proano D, Moharrami M, Kaura Km, et al. Environmental scan of publicly financed dental care in Canada: 2022 update. Toronto (ON): University of Toronto, Faculty of Dentistry, Dental Public Health; 2022. Available: https://caphd.ca/wp-content/uploads/2022/10/Canada-Dental-environmentscan-UofT-20221017.pdf (accessed 2023 Jan 14).
- World Health Organization. Global strategy and action plan on oral health 2023–2030. Geneva (Switzerland): The Organization; 2024. Available: https://www.who.int/publications/i/item/9789240090538 (accessed 2025 Jun 4).
- Harnagea H, Lamothe L, Couturier Y, Esfandiari S, Voyer R, Charbonneau A, et al. From theoretical concepts to policies and applied programmes: the landscape of integration of oral health in primary care. BMC Oral Health. 2018;18:23. doi: 10.1186/s12903-018-0484-8
- McNeil DW, Pereira DB, Ensz OS, Lukose K, Harrell G, Feller DB. Toward a comprehensive model of medical-dental-behavioral integration. JDR Clin Transl Res. 2024;9(1 Suppl):23S-31S. doi: 10.1177/23800844241273836
- Raju K, Thakur YB, Garell C, Hilton IV. Medical-dental integration: a promising approach to address unmet dental needs of children and youth with special health care needs. J Calif Dental Assoc. 2022;50(6):331-43. doi: 10.1080/19424396.2022.12220721
- Grantmakers in Health (GIH). Issue Brief 40: Returning the mouth to the body: integrating oral health & primary care. Washington (DC): GIH; 2012. Available: https://www.gih.org/files/FileDownloads/Returning_the_Mouth_to_the_Body_no40_September_2012.pdf (accessed 2023 Jun 21).
- Tiwari T, Kondratenko MA, Nasiha N, Stobbs-Vergara J, Callanan D, Johnson LR, et al. Medical-dental integration models: a critical review of the last decade. Aurora (CO): University of Colorado Anschutz, Delta Dental Institute; 2022. Available: https://www.deltadentalinstitute.com/content/dam/delta-dental-policy/pdf/UCO_MDI_White_Paper.pdf (accessed 2023 Jun 2).
- Bhuiya A, Scallan E, Alam S, Sharma K, Wilson MG. Rapid synthesis: identifying the features and impacts of community health centres. Hamilton (ON): McMaster Health Forum; 2020. Available: https://www.mcmasterforum.org/docs/default-source/product-documents/rapid-responses/identifying-the-features-and-impacts-of-community-health-centres.pdf?sfvrsn=234559d5_3#:~:text=CHCs%20helped%20address%20health%2Dequity,and%20management%20of%20chronic%20conditions (accessed 2023 Aug 2).
- British Columbia Association of Community Health Centres. About CHCs. The Association; n.d. Available: https://bcachc.org/about-chcs/ (accessed 2023 Oct 1).
- Langelier M, Surdu S, Goodwin N. Case studies of 6 safety net organizations that integrate oral and mental/behavioral health with primary care services. Rensselaer (NY): State University of New York, Oral Health Workforce Research Center; 2019. Available: https://www.chwsny.org/wp-content/uploads/2019/02/OHWRC_Case_Studies_Oral_and_Behavioral_Health_Integration_With_Primary_Care_2019.pdf (accessed 2024 May 20).
- Gupta A, Akiya K, Glickman R, Silver D, Pagan JA. How patient-centered medical homes integrate dental services into primary care: a scoping review. Med Care Res Rev. 2022;79(4):487-99. doi: 10.1177/10775587211030376
- Wong ST, MacDonald M, Valaitis RK, Kaczorowski J, Munroe V, Blatherwick J. An environmental scan of primary care and public health in the province of British Columbia: a series report. Vancouver (BC): University of British Columbia, Centre for Health Services and Policy Research; 2009. Available: https://open.library.ubc.ca/soa/cIRcle/collections/facultyresearchandpublications/52383/items/1.0048529 (accessed 2026 Mar 4).
- Charlton P, Doucet S, Azar R, Nagel DA, Boulos L, Luke A, et al. The use of the environmental scan in health services delivery research: a scoping review protocol. BMJ Open. 2019;9(9):e029805. doi: 10.1136/bmjopen-2019-029805
- Charlton P, Kean T, Liu RH, Nagel DA, Azar R, Doucet S, et al. Use of environmental scans in health services delivery research: a scoping review. BMJ Open. 2021;11(11):e050284. doi: 10.1136/bmjopen-2021-050284
- Choo CW. Environmental scanning as information seeking and organizational learning. Inf Res. 2001;7(1):1-26. Available: https://informationr.net/ir/7-1/paper112.html (accessed 2025 Sep 11).
- Johnson JL, Adkins D, Chauvin S. A review of the quality indicators of rigor in qualitative research. Am J Pharm Educ. 2020;84(1):7120. doi: 10.5688/ajpe7120
- McKernan SC, Kuthy R, Tuggle L, Garcia DT. Medical-dental integration in public health settings: an environmental scan. Iowa City (IA): University of Iowa, Public Policy Center; 2018. Available: https://iro.uiowa.edu/esploro/outputs/report/9983557186402771 (accessed 2022 Nov 6).
- Pourat N, Martinez AE, Haley LA, Crall JJ. Colocation does not equal integration: identifying and measuring best practices in primary care integration of children’s oral health services in health centers. J Evid Based Dent Pract. 2020;20(4):101469. doi: 10.1016/j.jebdp.2020.101469
- British Columbia Association of Community Health Centres. Member survey report. The Association; 2021. Available: https://bcachc.org/wp-content/uploads/2021/04/MemberSurveyReport_1.5.pdf (accessed 2022 Jan 2).
- National Network for Oral Health Access. User’s guide for the implementation of the oral health core clinical competencies. Version 2. Denver (CO): The Network; 2024. Available: https://drive.google.com/file/d/1Ms5EF918NvHvdxnkSaJdIEH-YkhNvkcp/view (accessed 2024 Jul 4).
- Harnagea H, Couturier Y, Shrivastava R, Girard F, Lamothe L, Bedos CP, et al. Barriers and facilitators in the integration of oral health into primary care: a scoping review. BMJ Open. 2017;7(9):e016078. doi: 10.1136/bmjopen-2017-016078
- Nelson S, Kim EGR, Kaelber DC. Integrating oral health into primary care: perspectives for older adults. J Dent Res. 2023;102(8):849-53. doi: 10.1177/00220345231165011
- Pourat N, Martinez AE, Crall JJ. Better together: co-location of dental and primary care provides opportunities to improve oral health. Policy Brief UCLA Cent Health Policy Res. 2015;PB2015-4:1-8. PMID: 26591904
- Longhurst A, Cohen M. The importance of community health centres in BC’s primary care reforms: what the research tells us. Vancouver (BC): Canadian Centre for Policy Alternatives, BC Office; 2019. Available: https://www.policyalternatives.ca/wp-content/uploads/attachments/ccpa-bc_march2019_chcs-in-bc.pdf (accessed 2021 Jan 10).
- Office of the Premier. B.C. government’s primary health-care strategy focuses on faster, team-based care [news release]. Victoria (BC): Government of British Columbia; 2018. Available: https://news.gov.bc.ca/releases/2018PREM0034-001010 (accessed 2024 Jul 24).
- British Columbia Association of Community Health Centres. Community health centres in British Columbia: starter kit. The Association; n.d. Available: https://bcachc.org/wp-content/uploads/2023/03/BCACHC_CHC-Starter-Kit_2022-23_Final.pdf (accessed 2024 Jul 10).
- Emami E. The integration of oral health in primary care: interdisciplinary research initiative. Mosaic. 2015;7:6-7. Available: https://caphd.ca/wp-content/uploads/2022/06/Mosaic_Spring_2015.pdf (accessed 2025 Jan 30).
- Maxey HL. Integration of oral health with primary care in health centers: profiles of five innovative models. Bethesda (MD): National Association of Community Health Centers; n.d. Available: https://hdl.handle.net/1805/7074 (accessed 2024 Jan 12).
- Maxey HL, Norwood CW, Liu Z. State policy environment and the dental safety net: a case study of professional practice environments’ effect on dental service availability in Federally Qualified Health Centers. J Public Health Dent. 2016;76(4):295-302. doi: 10.1111/jphd.12155
- Government of Canada. Canadian dental care plan. Ottawa (ON): Government of Canada; 2023. Available: https://www.canada.ca/en/services/benefits/dental/dental-care-plan.html (accessed 2025 Feb 5).